Counseling Psychology and Psychotherapy
2022. Vol. 30, no. 1, 67–92
doi:10.17759/cpp.2022300105
ISSN: 2075-3470 / 2311-9446 (online)
Pathways Through Coping Strategies to Psychological Symptoms: Structural Equation Modeling That Highlights the Importance of Social Support
Abstract
General Information
Keywords: structural equation modeling (SEM), engagement coping strategies, disengagement coping strategies, psychological symptoms
Journal rubric: Empirical Researches
Article type: scientific article
DOI: https://doi.org/10.17759/cpp.2022300105
Received: 21.10.2020
Accepted:
For citation: Schetsche C. Pathways Through Coping Strategies to Psychological Symptoms: Structural Equation Modeling That Highlights the Importance of Social Support. Konsul'tativnaya psikhologiya i psikhoterapiya = Counseling Psychology and Psychotherapy, 2022. Vol. 30, no. 1, pp. 67–92. DOI: 10.17759/cpp.2022300105.
Full text
Lazarus’ and Folkman’s [20] transactional model describes stress as an interaction between an individual and his/her environment. Stress would appear when an individual perceives his/her resources as scarce and insufficient to cope with the demands of the environment. In other words, stress is a dynamic concept and reflects the perceived discrepancies between the demands of the environment and the available resources to deal with them. The key to the model lies in the cognitive evaluation of both the stimulus and the response, and in this regard, Lazarus [19] differentiated between problem-oriented coping strategies and emotion-oriented coping strategies.
Through hierarchical factor analysis, Tobin [39] organized eight primary first-order coping strategies into two higher-order categories: engagement and disengagement strategies and, within each of these categories, they differentiated between emotion- and problem-focused strategies. While engagement strategies (e.g., cognitive restructuring, problem solving, and social support) include an active effort to manage stressful situations, disengagement strategies (e.g., self-criticism, wishful thinking, problem avoidance and emotional concealment) are characterized by behaviors and thoughts that do not intend to modify the situation.
Numerous studies analyzing the relationship between coping strategies and psychological symptoms have shown that the use of engagement strategies reduces the likelihood of disengagement, or avoidance, coping strategies. In this sense, Compas et al. [8] emphasize that the coping process is multidimensional, so they do not recommend the use of higher-order factor models but primary first-order coping strategies. They also highlight the difference between voluntary and involuntary responses to a stressful situation. Within each of these two categories, Connor-Smith et al. [10] differentiate between approach and avoidance strategies, but other studies show that avoidance strategies could operate, in general, as involuntary responses [4; 15].
Finally, a meta-analysis carried out by Compas et al. [9] should be mentioned. On the one hand, they confirm that disengagement coping strategies are related to higher levels of pathological symptoms and, on the other hand, they criticize the current state of research on emotional regulation and coping strategies. The authors state that there is a stagnation in the conceptualization and development of methods that can create a link between the two concepts.
Present Study
The objective of the present study was to determine the causal relationships between the coping strategies and to relate them to psychological symptoms. Although there are indeed studies that used structural equation modeling to develop causal models [1; 25; 29; 34], these used higher-order factor models, while models that included a wide variety of primary first-order strategies have not been found. Following Compas’ et al. [9] indications for future research, the second objective was to determine which engagement strategies are most effective in reducing the probability of using emotional suppression. The third objective consisted in determining the effects that psychological symptoms could have on the use of coping strategies.
Method
Sample and Procedure
For data collection, a G-Suite account of the Google Forms© digital platform was used. This account guarantees compliance with the General Data Protection Regulation and, in this way, ensures the confidential treatment of the participants’ information. The first page of the questionnaire informed the participants of the possibility of withdrawing at any time and included a contact email. After receiving an informed consent for participation, the questionnaires were presented. The recruitment of participants was carried out through the social network «Facebook» and, to ensure satisfactory completion of the survey, a pilot test was carried out with 30 individuals.
Table 1 represents the sociodemographic data of the non-probabilistic sample, which was collected in Germany, between April 14 and May 5, 2020. Concerning educational level, it was striking to find a large number of participants with more than 16 years of study, since only 17.6% of the German population has had university studies [35].
Instruments
ICD-10-Symptom Rating (ISR)
Symptoms were measured through the ICD-10-Symptom-Rating (ISR) by Tritt et al. [40]. It consists of 29 items, rated on a 5-point Likert scale (0 =does not apply to 4 = applies extremely), and it covers five main dimensions: depressive syndrome (4 items); anxiety syndrome (4 items); obsessive-compulsive syndrome (3 items); somatoform syndrome (3 items); eating disorder (3 items); an additional dimension to carry out a screening of other conditions, such as suicidality, post-traumatic stress disorder, etc. (12 items), and an overall score that covers all symptoms. The instrument has internal consistencies between 0.86 ≥ α ≥ 0.78.
Table 1
|
Sociodemographic characteristics (N = 295) |
|||||
|
|
|||||
|
|
Gender |
Total |
|||
|
Female |
Male |
Other |
|||
|
Age |
|
||||
|
|
Mean |
48.56 |
53.68 |
47.75 |
49.87 |
|
SD |
14.74 |
16.32 |
12.18 |
15.26 |
|
|
Civil status |
|
||||
|
|
Single |
54 |
16 |
2 |
72 |
|
|
Married / Domestic partner |
119 |
51 |
0 |
170 |
|
|
Divorced / Separated |
38 |
8 |
2 |
48 |
|
|
Widower |
4 |
1 |
0 |
5 |
|
Education |
|||||
|
|
6—10 years |
14 |
4 |
1 |
19 |
|
|
11—15 years |
63 |
13 |
0 |
76 |
|
|
16—20 years |
132 |
49 |
3 |
184 |
|
|
More than 20 years |
6 |
10 |
0 |
16 |
|
Total |
215 |
76 |
4 |
295 |
|
Notes. SD, Standard deviation.
Coping Strategies Inventory (CSI)
The Coping Strategies Inventory (CSI) by Tobin et al. [39] represents a hierarchical factor model. The third-order model comprises two strategies (engagement and disengagement strategies) and the second-order model comprises four strategies, which consist of eight first-order primary coping strategies: (1) Problem engagement: problem solving and cognitive restructuring; (2) Emotion engagement: social support and express emotions; (3) Problem disengagement: problem avoidance and wishful thinking; (4) Emotion disengagement: social withdrawal and self-criticism.
The descriptions of the eight primary strategies are as follows. Problem solving: Cognitive and behavioral strategies that aim at eliminating stress by modifying the situation that produces it; Cognitive restructuring: Cognitive strategies that modify the meaning of the stressful situation; Social support: Strategies related to seeking for emotional support; Express emotions: Strategies that aim at releasing the emotions that occur under stress; Problem avoidance: Strategies that include denial and avoidance of thoughts or actions related to the stressful event; Wishful thinking: Cognitive strategies that reflect a wish for reality not to be stressful; Social withdrawal: Withdrawal from friends, family, colleagues and significant others; Self-criticism: Strategies based on self-blame and self-criticism for the occurrence of a stressful situation or its inappropriate handling.
Cano García et al. [5] validated and adapted this instrument to the Spanish-speaking context. During this process, they could reduce the instrument to 40 items. A 5-point Likert scale (0 = not at all to 4 = completely) is used for answers and the internal consistencies are between 0.89 ≥ α ≥ 0.63.
In this study, a German adaptation (CSI-26 — 9F) of the brief version by Cano García et al. [5] was used. This instrument includes an additional dimension, emotional concealment, which serves to increase differentiation between the coping strategies. At the time of this publication, the article on the German adaptation of the instrument has been under editorial review.
Data Analysis
MVN package [17] was used to calculate multivariate normality, and MASS package [42] was used to detect multivariate outliers. Structural equation modeling (SEM), meaning the development of the model, the model fit, the calculation of the effects, and the measurement invariance analyses, was carried out with the help of the lavaan package [31]. The packages mentioned are part of the Core Team’s [12] R software. Items from the psychometric instruments were not used to develop the model, but rather the factors which were proposed by their authors. For all the calculations mentioned, the probability value p ≤ 0.05 was used.
Results
The robust Minimum Covariance Determinant test [22] was carried out to detect multivariate outliers. 17 values were classified as severe outliers (observations numbered 19, 25, 50, 63, 74, 75, 79, 82, 91, 129, 137, 161, 171, 179, 191, 244, 271), so they were removed from the sample, leaving the total at 278.
In Table 2, we can see the descriptive statistics and the internal consistencies of the psychometric instruments that were used. Regarding the CSI-26 — 9F, social support and problem solving can be highlighted as the strategies with the highest mean and self-criticism and problem avoidance as the strategies with the lowest means. As far as the ISR is concerned, depression, anxiety, and somatoform disorder emerged as the least pronounced symptoms. Also, the latter had a kurtosis that was above ± 2, so it did not have a normal distribution according to Hinton [13]. Following Hinton’s classification, all the values of internal consistencies were between moderate and high.
The absence of multicollinearity was verified and, through the use of Mardia’s test [23], it was found that the factors did not represent multivariate normality, so the model fits were evaluated using the Satorra-Bentler scaled chi-square (S-Bχ2) [32], thus complying with the requirements established for the use of the Maximum Likelihood Method, or MLM [14, 44]. Furthermore, the Satorra and Bentler adjustments [32] also allow for the calculation of a robust standard error and significance value.
Taking into account the aforementioned non-compliance with multivariate normality, not only the Root Mean Square Error of Approximation (RMSEA) and Comparative Fit Index (CFI) were verified, but also Nonnormed Fit Index (NNFI). Due to the sample size ≤ 500, Standardized Root Mean Square Residual (SRMR) values were not interpreted, but only those mentioned above [16]. According to Hu and Bentler’s indications [14], a model can be considered as adequate when its model fit takes the following values: χ2 / df ≤ 3, RMSEA ≤ 0.06, CFI ≥ 0.95, NNFI ≥ 0.95, although other authors, such as Marsh et al. [24], highlight the importance of evaluating the sample size and the complexity of the model. Following the research of these authors, RMSEA and NNFI should be used to evaluate a complex model at a sample size of N = 250.
As far as regression analyses and the presence of data that do not comply with multivariate normality are concerned, Preacher and Hayes [28] suggest using the bootstrapping method to evaluate the indirect effects. This method was therefore used to establish confidence intervals. Within the context of structural equation models, bootstrapping allows to evaluate the stability of the model parameters and to estimate a great variety of other measures [16; 36; 45]. The use of the Satorra and Bentler adjustment [32], together with the bootstrapping method, allowed to calculate the regressions not only with robust standard errors but also with confidence intervals.
Table 2
|
Descriptive statistics and internal consistencies of ISR y CSI-26 — 9F (N = 278) |
|||||||||
|
|
Items |
M |
Mdn |
SD |
Min |
Max |
Skew |
Kurtosis |
α |
|
Problem solving |
3 |
2.83 |
3.00 |
0.67 |
0.00 |
4.00 |
-0.57 |
0.75 |
0.68 |
|
Cognitive restructuring |
3 |
2.55 |
2.67 |
0.76 |
0.33 |
4.00 |
-0.56 |
0.04 |
0.71 |
|
Express emotions |
3 |
1.70 |
1.67 |
0.90 |
0.00 |
4.00 |
0.19 |
-0.43 |
0.85 |
|
Social support |
3 |
2.80 |
3.00 |
0.80 |
0.00 |
4.00 |
-0.50 |
-0.18 |
0.68 |
|
Problem avoidance |
3 |
0.91 |
0.67 |
0.74 |
0.00 |
3.00 |
0.65 |
-0.24 |
0.70 |
|
Wishful thinking |
3 |
2.35 |
2.33 |
1.04 |
0.00 |
4.00 |
-0.22 |
-0.73 |
0.82 |
|
Self-criticism |
3 |
0.91 |
0.67 |
0.77 |
0.00 |
3.00 |
0.61 |
-0.45 |
0.77 |
|
Social withdrawal |
2 |
2.06 |
2.00 |
1.01 |
0.00 |
4.00 |
0.09 |
-0.61 |
0.63 |
|
Emotional concealment |
3 |
1.24 |
1.00 |
0.87 |
0.00 |
3.67 |
0.48 |
-0.38 |
0.84 |
|
Depression |
4 |
1.12 |
1.00 |
0.86 |
0.00 |
4.00 |
0.87 |
0.28 |
0.85 |
|
Anxiety |
4 |
1.00 |
0.75 |
0.86 |
0.00 |
4.00 |
0.95 |
0.11 |
0.78 |
|
Obsessive-compulsive disorder |
3 |
0.74 |
0.33 |
0.80 |
0.00 |
3.00 |
0.72 |
-0.64 |
0.64 |
|
Somatoform disorder |
3 |
0.41 |
0.00 |
0.60 |
0.00 |
2.67 |
1.64 |
2.41 |
0.69 |
|
Eating disorder |
3 |
0.87 |
0.67 |
0.86 |
0.00 |
3.33 |
0.83 |
-0.25 |
0.73 |
|
ISR Overall score |
29 |
0.78 |
0.66 |
0.49 |
0.00 |
2.43 |
0.72 |
-0.19 |
0.89 |
Taking into account the aforementioned non-compliance with multivariate normality, not only the Root Mean Square Error of Approximation (RMSEA) and Comparative Fit Index (CFI) were verified, but also Nonnormed Fit Index (NNFI). Due to the sample size ≤ 500, Standardized Root Mean Square Residual (SRMR) values were not interpreted, but only those mentioned above [16]. According to Hu and Bentler’s indications [14], a model can be considered as adequate when its model fit takes the following values: χ2 / df ≤ 3, RMSEA ≤ 0.06, CFI ≥ 0.95, NNFI ≥ 0.95, although other authors, such as Marsh et al. [24], highlight the importance of evaluating the sample size and the complexity of the model. Following the research of these authors, RMSEA and NNFI should be used to evaluate a complex model at a sample size of N = 250.
As far as regression analyses and the presence of data that do not comply with multivariate normality are concerned, Preacher and Hayes [28] suggest using the bootstrapping method to evaluate the indirect effects. This method was therefore used to establish confidence intervals. Within the context of structural equation models, bootstrapping allows to evaluate the stability of the model parameters and to estimate a great variety of other measures [16; 36; 45]. The use of the Satorra and Bentler adjustment [32], together with the bootstrapping method, allowed to calculate the regressions not only with robust standard errors but also with confidence intervals.
First Step: Direct Effects of Coping Strategies on Symptoms
The strategies that had a direct effect on symptoms were analyzed first. In Table 3, we can see the significant effects. None of the coping strategies had a direct effect on somatoform disorder, so it was not included in this table. Of the nine coping strategies, only five had a direct effect on symptoms: problem solving, wishful thinking, self-criticism, social withdrawal, and emotional concealment. Of these strategies, self-criticism is highlighted for being the only one with direct effects on all symptoms, and social withdrawal for having direct effects on three symptoms. Furthermore, problem solving was the only strategy with a negative effect on symptoms, and therefore the only strategy with a direct effect that improved symptoms.
Table 3
|
Regression results using symptoms as criteria and coping strategies as predictors (N = 278) |
||||||||
|
|
|
|
95% CI |
|
|
|
|
|
|
Criterion |
Predictors |
b |
LL |
UL |
SE B |
z |
Beta (β) |
p |
|
ISR Overall score |
||||||||
|
|
Problem solving |
-0.122 |
-0.211 |
-0.032 |
0.046 |
-2.671 |
-0.164** |
0.008 |
|
|
Wishful thinking |
0.089 |
0.036 |
0.143 |
0.027 |
3.277 |
0.187** |
0.001 |
|
|
Self-criticism |
0.132 |
0.068 |
0.195 |
0.032 |
4.061 |
0.205** |
0.000 |
|
|
Social withdrawal |
0.089 |
0.035 |
0.143 |
0.028 |
3.231 |
0.182** |
0.001 |
|
|
Emotional concealment |
0.094 |
0.017 |
0.171 |
0.039 |
2.403 |
0.165* |
0.016 |
|
Depression |
||||||||
|
Problem solving |
-0.224 |
-0.383 |
-0.065 |
0.081 |
-2.763 |
-0.174** |
0.006 |
|
|
Wishful thinking |
0.165 |
0.074 |
0.256 |
0.046 |
3.570 |
0.200** |
0.000 |
|
|
Self-criticism |
0.164 |
0.051 |
0.276 |
0.057 |
2.853 |
0.147** |
0.004 |
|
|
Social withdrawal |
0.126 |
0.035 |
0.218 |
0.047 |
2.706 |
0.149** |
0.007 |
|
|
Emotional concealment |
0.170 |
0.033 |
0.306 |
0.070 |
2.434 |
0.172* |
0.015 |
|
|
Anxiety |
||||||||
|
Problem solving |
-0.217 |
-0.373 |
-0.061 |
0.080 |
-2.727 |
-0.168** |
0.006 |
|
|
Wishful thinking |
0.150 |
0.052 |
0.248 |
0.050 |
3.001 |
0.180** |
0.003 |
|
|
Self-criticism |
0.176 |
0.036 |
0.316 |
0.071 |
2.459 |
0.157* |
0.014 |
|
|
Social withdrawal |
0.123 |
0.015 |
0.230 |
0.055 |
2.243 |
0.144* |
0.025 |
|
|
Obsessive-compulsive disorder |
||||||||
|
Self-criticism |
0.161 |
0.032 |
0.289 |
0.065 |
2.457 |
0.155* |
0.014 |
|
|
Social withdrawal |
0.106 |
0.001 |
0.211 |
0.054 |
1.976 |
0.134* |
0.048 |
|
|
Eating disorder |
||||||||
|
Self-criticism |
0.172 |
0.017 |
0.328 |
0.079 |
2.168 |
0.153* |
0.030 |
|
Notes. ** p <0.01; * p <0.05; CI, confidence interval; LL, lower limit; US, upper limit; robust SE and p values with Satorra-Bentler adjustments.
Second Step: Direct Effects between Coping Strategies
Having identified the strategies with direct effects on symptoms (problem solving, wishful thinking, self-criticism, social withdrawal, and emotional concealment), the direct effects on these five by other strategies were analyzed. Table 4 represents the significant direct effects among all coping strategies.
Table 4
|
Regression results using each coping strategy as a criterion (N = 278) |
||||||||
|
|
|
|
95% CI |
|
|
|
|
|
|
Criterion |
Predictors |
b |
LL |
UL |
SE B |
z |
Beta (β) |
p |
|
Problem solving |
|
|
|
|
|
|
||
|
|
Cognitive restructuring |
0.166 |
0.049 |
0.283 |
0.060 |
2.772 |
0.249** |
0.006 |
|
|
Social support |
0.115 |
0.005 |
0.226 |
0.056 |
2.048 |
0.173* |
0.041 |
|
Problem avoidance |
-0.203 |
-0.325 |
-0.081 |
0.062 |
-3.262 |
-0.305** |
0.001 |
|
|
Wishful thinking |
-0.075 |
-0.145 |
-0.004 |
0.036 |
-2.073 |
-0.112* |
0.038 |
|
|
Cognitive restructuring |
||||||||
|
|
Problem solving |
0.214 |
0.076 |
0.353 |
0.071 |
3.037 |
0.283** |
0.002 |
|
Problem avoidance |
0.309 |
0.183 |
0.434 |
0.064 |
4.832 |
0.408** |
0.000 |
|
|
Social withdrawal |
-0.102 |
-0.197 |
-0.006 |
0.049 |
-2.090 |
-0.135* |
0.037 |
|
|
Express emotions |
||||||||
|
Social support |
0.167 |
0.071 |
0.373 |
0.072 |
2.319 |
0.185* |
0.020 |
|
|
Problem avoidance |
0.222 |
0.071 |
0.373 |
0.077 |
2.885 |
0.247** |
0.004 |
|
|
Self-criticism |
0.249 |
0.120 |
0.378 |
0.066 |
3.776 |
0.276** |
0.000 |
|
|
Emotional concealment |
-0.345 |
-0.482 |
-0.209 |
0.070 |
-4.953 |
-0.383** |
0.000 |
|
|
Social support |
||||||||
|
|
Problem solving |
0.141 |
0.014 |
0.268 |
0.065 |
2.177 |
0.117* |
0.030 |
|
|
Express emotions |
0.114 |
0.023 |
0.206 |
0.047 |
2.460 |
0.143* |
0.014 |
|
|
Wishful thinking |
0.100 |
0.018 |
0.183 |
0.042 |
2.376 |
0.125* |
0.018 |
|
Social withdrawal |
-0.190 |
-0.280 |
-0.100 |
0.046 |
-4.142 |
-0.237** |
0.000 |
|
|
Emotional concealment |
-0.290 |
-0.408 |
-0.172 |
0.060 |
-4.816 |
-0.361** |
0.000 |
|
|
Problem-avoidance |
||||||||
|
Problem solving |
-0.205 |
-0.333 |
-0.077 |
0.065 |
-3.144 |
-0.186** |
0.002 |
|
|
Cognitive restructuring |
0.241 |
0.142 |
0.339 |
0.050 |
4.800 |
0.248** |
0.000 |
|
|
Express emotions |
0.126 |
0.041 |
0.212 |
0.044 |
2.886 |
0.155** |
0.004 |
|
|
Self-criticism |
0.169 |
0.058 |
0.280 |
0.057 |
2.989 |
0.177** |
0.003 |
|
|
Emotional concealment |
0.303 |
0.191 |
0.415 |
0.057 |
5.298 |
0.357** |
0.000 |
|
|
Wishful thinking |
||||||||
|
|
Problem solving |
-0.192 |
-0.377 |
-0.007 |
0.094 |
-2.031 |
-0.123* |
0.042 |
|
Cognitive restructuring |
-0.196 |
-0.391 |
-0.002 |
0.099 |
-1.978 |
-0.144* |
0.048 |
|
|
Social support |
0.211 |
0.031 |
0.391 |
0.092 |
2.296 |
0.163* |
0.022 |
|
|
Social withdrawal |
0.202 |
0.065 |
0.340 |
0.070 |
2.894 |
0.198** |
0.004 |
|
|
Self-criticism |
||||||||
|
Express emotions |
0.183 |
0.092 |
0.275 |
0.047 |
3.924 |
0.215** |
0.000 |
|
|
Problem avoidance |
0.219 |
0.083 |
0.356 |
0.070 |
3.153 |
0.209** |
0.002 |
|
|
Social withdrawal |
-0.093 |
-0.178 |
-0.008 |
0.043 |
-2.146 |
-0.122* |
0.032 |
|
|
Emotional concealment |
0.235 |
0.107 |
0.363 |
0.065 |
3.607 |
0.265** |
0.000 |
|
|
Social withdrawal |
||||||||
|
Cognitive restructuring |
-0.175 |
-0.343 |
-0.007 |
0.086 |
-2.047 |
-0.131* |
0.041 |
|
|
Social support |
-0.347 |
-0.511 |
-0.184 |
0.083 |
-4.161 |
-0.276** |
0.000 |
|
|
Wishful thinking |
0.175 |
0.056 |
0.295 |
0.061 |
2.871 |
0.180** |
0.004 |
|
|
Self-criticism |
-0.158 |
-0.299 |
-0.017 |
0.072 |
-2.195 |
-0.120* |
0.028 |
|
|
Emotional concealment |
||||||||
|
Express emotions |
-0.230 |
-0.321 |
-0.139 |
0.047 |
-4.929 |
-0.239** |
0.000 |
|
|
Social support |
-0.281 |
-0.390 |
-0.173 |
0.055 |
-5.075 |
-0.261** |
0.000 |
|
|
Problem avoidance |
0.355 |
0.221 |
0.489 |
0.068 |
5.203 |
0.301** |
0.000 |
|
|
Self-criticism |
0.213 |
0.101 |
0.324 |
0.057 |
3.735 |
0.189** |
0.000 |
|
Notes. ** p <0.01; * p <0.05; CI, confidence interval; LL, lower limit; US, upper limit; robust SE and p values with Satorra-Bentler adjustments.
Due to a high number of direct effects, only those with a significance level of p ≤ 0.01 were selected. Analyzing this data, we found it striking that there were several direct effects of a reciprocal nature. Byrne [3] states that while it is true that there may be some legitimate reciprocal paths, not all paths may be of a substantial interest for a study. For this reason, the author suggests focusing on a flow that presents interest for the study. The main focus of the present study was to identify which of the engagement strategies, according to Tobin et al. [39] were most suitable to reduce the probability that disengagement strategies were used. Thus, only the effects of engagement strategies on disengagement strategies were considered, hence the flow of interest in Figure 1 is from left to right. In case of direct effects between two engagement strategies or between two disengagement strategies, the stronger direct effect was taken into account.
Cognitive restructuring stood out from the direct effects with a significance level of p ≤ 0.05, since it had a positive effect both on problem avoidance and social withdrawal due to a negative effect on self-criticism.
Third Step: Establishment of the First Causal Model and Analysis of Modification Indices
Figure 1 represents the first causal model that was established based on the direct effects that were previously described. Problem solving, cognitive restructuring, social support, and express emotions were placed in the left margin of the figure to highlight the flow of interest in the model.
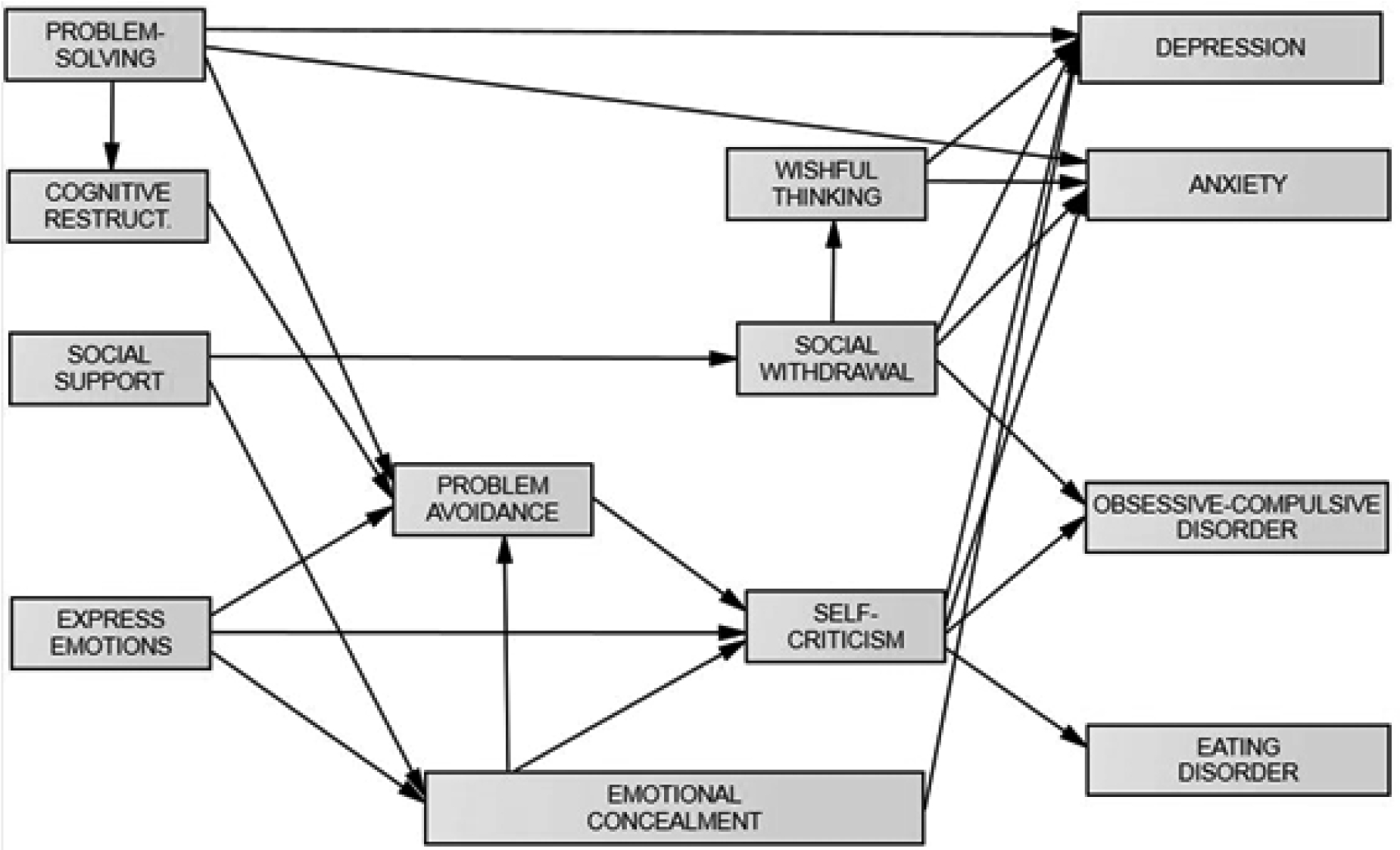
Fig. 1. First causal model with coping strategies and symptoms
From this moment, modification indices were used to improve the model fit, and six modifications were made. Table 5 represents the values taken by the respective model fit indices.
Table 5
|
Fit indices of the developed models (N = 278) |
||||||||
|
|
χ2 MLM |
df |
Scaling |
p |
RMSEA |
SRMR |
CFI |
NNFI |
|
Initial model |
78.284 |
45 |
1.019 |
0.000 |
0.052 |
0.064 |
0.942 |
0.902 |
|
Model after modification nº1 |
70.665 |
44 |
1.013 |
0.000 |
0.047 |
0.059 |
0.954 |
0.922 |
|
Model after modification nº2 |
63.095 |
43 |
1.014 |
0.024 |
0.041 |
0.054 |
0.965 |
0.940 |
|
Model after modification nº3 |
56.582 |
42 |
1.007 |
0.066 |
0.035 |
0.049 |
0.975 |
0.955 |
|
Model after modification nº4 |
50.883 |
41 |
1.007 |
0.139 |
0.030 |
0.048 |
0.983 |
0.969 |
|
Model after modification nº5 |
45.151 |
40 |
1.010 |
0.265 |
0.022 |
0.042 |
0.991 |
0.983 |
|
Final Model |
40.172 |
39 |
1.005 |
0.418 |
0.010 |
0.038 |
0.998 |
0.996 |
Notes. χ2 MLM — Scaled Chi-Square using maximum likelihood estimation with robust standard errors (MLM); df, Degrees of freedom; Scaling, Scaling correction factor for the Chi-Square from the Satorra-Bentler correction; RMSEA, Root Mean Square Error of Approximation; SRMR, Standardized Root Mean Square Residual; CFI, Comparative Fit Index; NNFI, Nonnormed Fit Index.
Multiple squared correlations were calculated, and it was determined that the developed model explained 21.9% of the variance in depression, 12.8% of the variance in anxiety, 5.7% of the variance in obsessive-compulsive disorder and 5.4% of the eating disorder variance. Figure 2 represents the final model with the four symptoms.
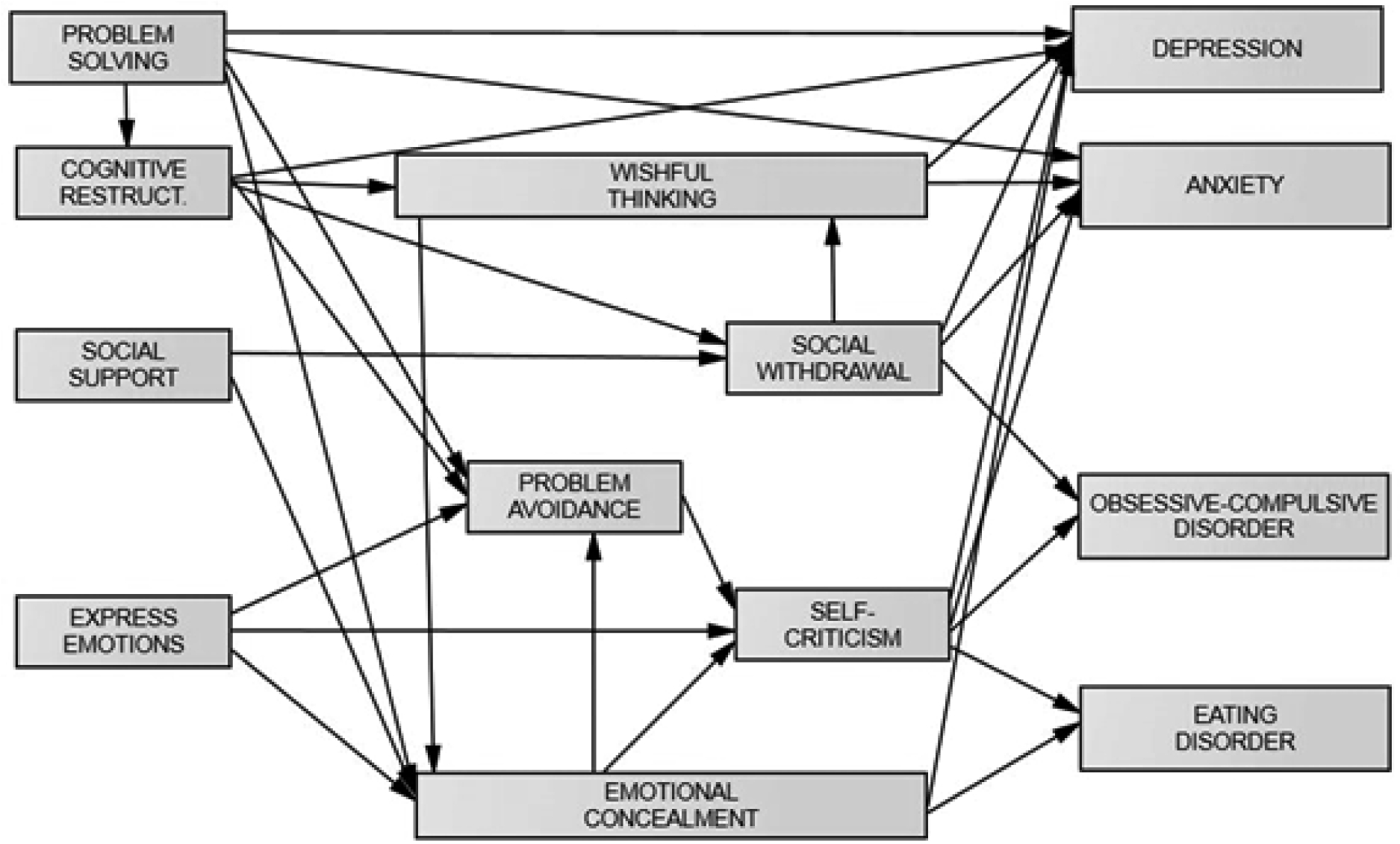
Fig. 2. Final causal model with coping strategies and symptoms
Table 6
|
Direct effects of the final model (N = 278) |
||||||||
|
|
|
|
95% CI |
|
|
|
|
|
|
Criterion |
Predictors |
b |
LL |
UL |
SE B |
z |
Beta (β) |
p |
|
Depression |
|
|
|
|
|
|
||
|
|
Self-criticism |
0.218 |
0.102 |
0.335 |
0.060 |
3.664 |
0.200** |
0.000 |
|
|
Problem solving |
-0.203 |
-0.325 |
-0.082 |
0.062 |
-3.277 |
-0.161** |
0.001 |
|
Wishful thinking |
0.133 |
0.054 |
0.211 |
0.040 |
3.319 |
0.163** |
0.001 |
|
|
|
Social withdrawal |
0.116 |
0.030 |
0.201 |
0.044 |
2.650 |
0.139** |
0.008 |
|
|
Emotional concealment |
0.123 |
0.027 |
0.219 |
0.049 |
2.505 |
0.127* |
0.012 |
|
|
Cognitive restructuring |
-0.123 |
-0.220 |
-0.026 |
0.050 |
-2.480 |
-0.111* |
0.013 |
|
Anxiety |
||||||||
|
Self-criticism |
0.198 |
0.063 |
0.333 |
0.069 |
2.873 |
0.178** |
0.004 |
|
|
Problem solving |
-0.179 |
-0.290 |
-0.068 |
0.057 |
-3.154 |
-0.139** |
0.002 |
|
|
Wishful thinking |
0.137 |
0.056 |
0.217 |
0.041 |
3.337 |
0.165** |
0.001 |
|
|
|
Social withdrawal |
0.135 |
0.036 |
0.235 |
0.051 |
2.674 |
0.159** |
0.008 |
|
Obsessive-compulsive disorder |
||||||||
|
Self-criticism |
0.197 |
0.077 |
0.317 |
0.061 |
2.674 |
0.189** |
0.001 |
|
|
Social withdrawal |
0.111 |
0.013 |
0.209 |
0.050 |
3.209 |
0.140** |
0.008 |
|
|
Eating disorder |
||||||||
|
Self-criticism |
0.168 |
0.024 |
0.311 |
0.073 |
2.294 |
0.150* |
0.022 |
|
|
Emotional concealment |
0.142 |
0.026 |
0.258 |
0.059 |
2.397 |
0.143* |
0.017 |
|
|
Cognitive restructuring |
||||||||
|
Problem solving |
0.210 |
0.063 |
0.357 |
0.075 |
2.793 |
0.185** |
0.005 |
|
|
Wishful thinking |
||||||||
|
Social withdrawal |
0.180 |
0.058 |
0.302 |
0.062 |
2.897 |
0.175** |
0.004 |
|
|
Cognitive restructuring |
-0.216 |
-0.395 |
-0.037 |
0.091 |
-2.361 |
-0.158* |
0.018 |
|
|
Social withdrawal |
||||||||
|
Social support |
-0.380 |
-0.524 |
-0.235 |
0.074 |
-5.148 |
-0.303** |
0.000 |
|
|
Cognitive restructuring |
-0.216 |
-0.376 |
-0.057 |
0.081 |
-2.661 |
-0.163** |
0.008 |
|
|
Self-criticism |
||||||||
|
Emotional concealment |
0.208 |
0.088 |
0.327 |
0.061 |
3.394 |
0.234** |
0.001 |
|
|
|
Problem avoidance |
0.203 |
0.073 |
0.333 |
0.066 |
3.065 |
0.195** |
0.002 |
|
Express emotions |
0.196 |
0.109 |
0.282 |
0.044 |
4.421 |
0.229** |
0.000 |
|
|
Emotional concealment |
||||||||
|
Express emotions |
-0.159 |
-0.263 |
-0.055 |
0.053 |
-2.992 |
-0.165** |
0.003 |
|
|
Social support |
-0.408 |
-0.517 |
-0.300 |
0.055 |
-7.378 |
-0.378** |
0.000 |
|
|
Wishful thinking |
0.105 |
0.026 |
0.184 |
0.040 |
2.609 |
0.125** |
0.009 |
|
|
Problem solving |
-0.160 |
-0.300 |
-0.020 |
0.071 |
-2.242 |
-0.123* |
0.025 |
|
|
Problem-avoidance |
||||||||
|
Express emotions |
0.158 |
0.072 |
0.244 |
0.044 |
3.613 |
0.194** |
0.000 |
|
|
Emotional concealment |
0.373 |
0.280 |
0.467 |
0.048 |
7.843 |
0.439** |
0.000 |
|
|
Cognitive restructuring |
0.242 |
0.141 |
0.342 |
0.051 |
4.730 |
0.248** |
0.000 |
|
|
|
Problem solving |
-0.204 |
-0.333 |
-0.074 |
0.066 |
-3.082 |
-0.184** |
0.002 |
Notes. ** p <0.01; * p <0.05; CI, confidence interval; LL, lower limit; US, upper limit; robust SE and p values with Satorra-Bentler adjustments.
Table 6 shows the direct effects of the final model. When analyzing its content, we were struck by the fact that the “express emotions” strategy appeared to have an ambiguous nature: On the one hand, it had a positive effect on self-criticism and problem avoidance and, on the other hand, it exerted a negative effect on emotional concealment. In the same way, it is worth highlighting cognitive restructuring: Although it had negative effects on wishful thinking and social withdrawal, it also had a positive effect on problem avoidance. The negative effect of social support on emotional concealment and the positive effect of emotional concealment on problem avoidance must also be highlighted since these were the strongest direct effects in the developed model.Lazarus’ and Folkman’s [20] transactional model describes stress as an interaction between an individual and his/her environment. Stress would appear when an individual perceives his/her resources as scarce and insufficient to cope with the demands of the environment. In other words, stress is a dynamic concept and reflects the perceived discrepancies between the demands of the environment and the available resources to deal with them. The key to the model lies in the cognitive evaluation of both the stimulus and the response, and in this regard, Lazarus [19] differentiated between problem-oriented coping strategies and emotion-oriented coping strategies.
In Table 7, we can see the matrix of the standardized total effects. Self-criticism, social withdrawal, and emotional concealment stood out as the strategies with the most significant effects on the symptoms analyzed. Regarding the engagement strategies, the effects of problem solving and social support must be emphasized. When analyzing the average of the total effects that the coping strategies had on each other, emotional concealment stood out as a mediator of the other disengagement strategies and, vice versa, social support was a moderator of the disengagement strategies.
Table 7
|
Matrix of standardized total effects (N = 278) |
|||||||||
|
|
Predictors |
||||||||
|
Criterions |
PRS |
COR |
SOS |
SOW |
WIT |
EXE |
EMC |
PRA |
SEC |
|
(1) Cognitive restructuring |
0.185 |
|
|
|
|
|
|
|
|
|
(2) Social withdrawal |
-0.030 |
-0.163 |
-0.303 |
||||||
|
(3) Wishful thinking |
-0.035 |
-0.187 |
-0.053 |
0.175 |
|||||
|
(4) Emotional concealment |
-0.127 |
-0.023 |
-0.385 |
0.022 |
0.125 |
-0.165 |
|||
|
(5) Problem avoidance |
-0.194 |
0.238 |
-0.169 |
0.010 |
0.055 |
0.122 |
0.439 |
||
|
(6) Self-criticism |
-0.068 |
0.041 |
-0.123 |
0.007 |
0.040 |
0.214 |
0.320 |
0.195 |
|
|
(7) Depression |
-0.221 |
-0.159 |
-0.124 |
0.172 |
0.187 |
0.022 |
0.191 |
0.039 |
0.200 |
|
(8) Anxiety |
-0.162 |
-0.049 |
-0.079 |
0.189 |
0.172 |
0.038 |
0.057 |
0.035 |
0.178 |
|
(9) Obsessive-compulsive disorder |
-0.017 |
-0.015 |
-0.066 |
0.141 |
0.008 |
0.040 |
0.060 |
0.037 |
0.189 |
|
(10) Eating disorder |
-0.028 |
0.003 |
-0.073 |
0.004 |
0.024 |
0.009 |
0.191 |
0.029 |
0.150 |
|
Mean of coping strategies (2—6) |
-0.045 |
-0.019 |
-0.206 |
0.053 |
0.073 |
0.057 |
0.379 |
0.195 |
- |
|
Mean of symptoms (7—10) |
-0.107 |
-0.055 |
-0.086 |
0.127 |
0.098 |
0.027 |
0.125 |
0.035 |
0.179 |
Notes. PRS, problem-solving; COR, cognitive restructuring; WIT, wishful thinking; SOS, social support; SOW, social withdrawal; PRA, problem-avoidance, SEC, self-criticism; EXE, express emotions; EMC, emotional concealment.
Fourth Step: Direct Effects of Symptoms on Coping Strategies
It was analyzed whether psychological symptoms could have any effect on coping strategies. Table 8 shows that depression had significant effects on cognitive restructuring and wishful thinking. Furthermore, the positive effect of obsessive-compulsive disorder on problem solving was evident.
To analyze whether the model was characterized by measurement invariance, a multiple-group analysis was performed taking the genders into account. This was limited to the female (n = 201) and male (n = 73) participants since only four individuals identified themselves as “other gender”. As Table 9 illustrates, the fit indices indicate a significantly accurate model for both genders.
Table 8
|
Regression results using coping strategies as criterion (N = 278) |
||||||||
|
|
|
|
95% CI |
|
|
|
|
|
|
Criterion |
Predictors |
b |
LL |
UL |
SE B |
z |
Beta (β) |
p |
|
Problem solving |
||||||||
|
|
Obsessive-compulsive disorder |
0.177 |
0.005 |
0.349 |
0.088 |
2.018 |
0.212* |
0.044 |
|
Cognitive restructuring |
||||||||
|
Depression |
-0.334 |
-0.560 |
-0.109 |
0.115 |
-2.908 |
-0.378** |
0.004 |
|
|
Wishful thinking |
||||||||
|
Depression |
0.348 |
0.042 |
0.655 |
0.156 |
2.230 |
0.288* |
0.026 |
|
Notes. ** p <0.01; * p <0.05; CI, confidence interval; LL, lower limit; US, upper limit; robust SE and p values with Satorra-Bentler adjustments.
Notes. PRS, problem-solving; COR, cognitive restructuring; WIT, wishful thinking; SOS, social support; SOW, social withdrawal; PRA, problem-avoidance, SEC, self-criticism; EXE, express emotions; EMC, emotional concealment.
Fourth Step: Direct Effects of Symptoms on Coping Strategies
It was analyzed whether psychological symptoms could have any effect on coping strategies. Table 8 shows that depression had significant effects on cognitive restructuring and wishful thinking. Furthermore, the positive effect of obsessive-compulsive disorder on problem solving was evident.
To analyze whether the model was characterized by measurement invariance, a multiple-group analysis was performed taking the genders into account. This was limited to the female (n = 201) and male (n = 73) participants since only four individuals identified themselves as “other gender”. As Table 9 illustrates, the fit indices indicate a significantly accurate model for both genders.
Table 9
|
Fit indices separated by gender (n = 274) |
||||||||
|
χ2 MLM |
df |
Scaling |
p |
RMSEA (90% CI) |
SRMR |
CFI |
NNFI |
|
|
Final model |
40.172 |
39 |
1.005 |
0.418 |
0.010 (0.000-0.043) |
0.038 |
0.998 |
0.996 |
|
Final model — Male |
44.564 |
39 |
0.977 |
0.249 |
0.044 (0.000-0.095) |
0.070 |
0.970 |
0.943 |
|
Final mo-del — Female |
32.392 |
39 |
1.006 |
0.764 |
0.000 (0.000-0.035) |
0.042 |
1.000 |
1.032 |
Notes. χ2 MLM — Scaled Chi-Square using maximum likelihood estimation with robust standard errors (MLM); df, Degrees of freedom; Scaling, Scaling correction factor for the Chi-Square from the Satorra-Bentler correction; RMSEA, Root Mean Square Error of Approximation; SRMR, Standardized Root Mean Square Residual; CFI, Comparative Fit Index; NNFI, Nonnormed Fit Index.
Table 10 represents the results of the multiple-group analysis. Following the Hu and Bentler [14] classification, all the models showed adequate values and, as far as the changes in the robust Chi-square indices were concerned, no significant differences were observed. Furthermore, the changes in the Comparative Fit Index (CFI) with ΔCFI ≥ -0.01 were within adequate ranges, according to Cheung and Rensvold [6].
Table 10
|
Model fit and model comparisons testing for measurement invariance (n = 274) |
|||||||||
|
Model |
Model fit |
|
|
Model comparisons |
|||||
|
|
S-B χ2 MLM |
df |
RMSEA |
CFI |
Δ S-B χ2 MLM |
Δdf |
p |
ΔRMSEA |
ΔCFI |
|
M1: Config. |
76.140 |
78 |
0.000 |
1.000 |
- |
- |
- |
- |
- |
|
M2: Weak |
76.777 |
78 |
0.000 |
1.000 |
0.637 |
0 |
- |
0.000 |
0.000 |
|
M3: Strong |
86.891 |
88 |
0.000 |
1.000 |
-10.114 |
10 |
0.431 |
0.000 |
0.000 |
|
M4: Strict |
101.690 |
98 |
0.017 |
0.993 |
-14.799 |
10 |
0.137 |
0.017 |
0.007 |
Notes. χ2 MLM — Scaled Chi-Square using maximum likelihood estimation with robust standard errors (MLM); df, Degrees of freedom; Scaling, Scaling correction factor for the Chi-Square from the Satorra-Bentler correction; RMSEA, Root Mean Square Error of Approximation; CFI, Comparative Fit Index.
Discussion
Pursuing the goals of determining causal relationships between coping strategies and evaluating their relationship with psychological symptoms, this study has been able to develop a significantly accurate model, which is characterized by measurement invariance for both genders. In line with the previous studies [8; 34], when taking into account the model as a whole, it became evident that the main function of the engagement strategies seemed to be to reduce the probability that disengagement strategies would appear, since the latter had the most considerable total effect on the symptoms.
Of the four engagement strategies, only problem solving and cognitive restructuring had direct effects on some symptoms. When considering the total effects on the symptoms, social support should also be highlighted. As far as the five disengagement strategies and their total effects on the symptoms are concerned, self-criticism, social withdrawal, and emotional concealment must be highlighted.
When analyzing the most substantial total effects that coping strategies had on each other, emotional concealment emerged as the most important mediator of the other disengagement strategies. This result is in line with Compas et al. [9] whose suggestion for future research gave rise to the second objective of the present study: to determine engagement strategies that were most effective in reducing probability of emotional suppression. Taking into account this objective, it was found that social support was both the strategy that had the most significant moderating effect on emotional concealment, and the strategy that had the most considerable moderating effect on all disengagement strategies. The fact that social support had the most substantial moderating effect on self-criticism, social withdrawal, and emotional concealment, with these three strategies having the most significant overall effect on the symptoms, is of particular importance.
The effects of social support have been studied in-depth, and Sommer and Fydrich [33] have already stated that it can increase self-esteem, motivation, hope for success, and reduce negative arousal and the perception of stress itself. In this way, social support positively modifies the perception of one’s own abilities, which could increase well-being and, as a consequence, make an individual tolerate, or overcome, future stressful experiences better. More recent studies reaffirm this: A meta-analysis not only demonstrated that social support predicted post-traumatic growth but also that this effect did not diminish in studies with longitudinal designs [27]. Park et al.[26] found an association between lack of social support and suicidal ideation, and a longitudinal study showed a positive correlation between social support and self-esteem [21]. Likewise, Budge et al. [2] emphasized the need to reduce avoidance coping strategies and increase social support since this could improve anxiety and depressive symptoms. Despite the results that underscore the positive effects of social support, possible negative associations should be considered. Within a broad meta-analysis, Compas et al. [9] also evaluated longitudinal studies and found a positive correlation between social support and some symptoms. These authors concluded that social support could be a maladaptive coping strategy when it takes the form of co-rumination. This behavior is characterized by talking with peers about a problem and frequently repeating the discussion on the same topic [37]. Another explanation could be that some symptoms have a positive association with the need for support: For example, high levels of depression were related to a greater need for support, especially when the need for support exceeded the social support received [30]. We could interpret this finding so that a long depressive episode could increase the need for support and, consequently, facilitate the search for social support.
In addition to the aforementioned results, it was found that both emotional expression and cognitive restructuring had an ambiguous nature. On the one hand, emotional expression decreased the probability of using emotional concealment and, on the other hand, it increased the probability that self-criticism and problem avoidance would be used. As to cognitive restructuring, it is worth noting that this strategy had the strongest total effect on wishful thinking, but it should also be borne in mind that cognitive restructuring mediated problem avoidance, that is, an attempt to forget about the problem. Three possible causes of this apparent contradiction were found in the literature. (1) Connor-Smith and Compas [11] highlight the need to differentiate between problem avoidance and distraction. Considering this view, we could infer that under certain circumstances problem avoidance may be an adequate strategy, since it provides the necessary space to carry out cognitive restructuring. This explanation would also be justified by their reciprocal associations: Cognitive restructuring had a direct effect on problem avoidance, and problem avoidance influenced cognitive restructuring. (2) The second possible cause lies in the nature of the stressor and its controllability since Troy et al. [41] and Christensen et al. [7] found that cognitive restructuring was related to higher levels of depressive symptoms when the stressor was controllable and to lower levels of depressive symptoms when the stressor was not controllable. If we consider point (1), we might intuit that, if there is a controllable stressor, some problem-avoidance is required to carry out cognitive restructuring. (3) The third cause that could explain the ambiguous nature of cognitive restructuring is based on the fact that depressive symptoms have a direct effect on it. If depression affects cognitive restructuring, this may lead to an increased use of problem avoidance.
If we now delve into the effects that psychological symptoms have on the use of coping strategies, we must highlight the negative effect that depression had on cognitive restructuring. Taking into account that depression is the most frequent psychological symptom [43], this negative effect on cognitive restructuring could be considered alarming.
Regarding disengagement strategies, we can point out social withdrawal as the only strategy that had unexpected characteristics. When performing the initial calculation of direct effects between the coping strategies, we found out that this strategy had an expected effect on depression, anxiety, and obsessive-compulsive disorder, and that it also had a moderating effect on self-criticism. As in case of cognitive restructuring, it is difficult to explain this finding, but, apparently, under certain circumstances, social withdrawal may also operate as an adaptive strategy. We could intuit that, when withdrawing socially, the number of situations in which the individual can feel him/herself responsible for the stressful situation decreases as well. Discussing this hypothesis, we can remember that Suls and Fletcher [38] analyzed the relative efficacy of avoidance strategies. According to their study, these strategies can reduce certain symptoms in the short term but not in the long term.
Taking into account the discussion above, we can highlight not only the need to treat social withdrawal and emotional concealment as separate constructs in the Coping Strategies Inventory but also the crucial importance of avoiding the use of higher-order factor models.
In addition, it should be mentioned that this study has failed to find direct effects on somatoform disorder. When relating this symptom to personality traits and thus complementing the Hierarchical Taxonomy of Psychopathology (HiTOP) model, Kotov et al. [18] encountered the same difficulty, so somatoform disorder appears to have a different nature than the other symptoms described in this study.
In order to determine the reasons why cognitive restructuring, emotional expression, and social withdrawal have the described ambiguous characteristics, it may be crucial to carry out an accurate study of personality traits and to include them in a causal model of coping strategies. Two other routes could include establishing a link between coping strategies and emotional regulation [9] and deepening research on stress controllability [7, 41]. Another possibility may be a combination of both: studying the controllability of stressors and their effect on emotional concealment and, following the results obtained in this study, studying the effects on social support.
Certain limitations and recommendations for future research should be underlined. First, it is important to bear in mind that non-probability sampling was carried out in the present study, and that the sample size can be considered relatively small, making it difficult to generalize the study results. Second, although it was possible to verify the measurement invariance across genders, it is important to keep in mind that this model is the first causal model that includes a high variety of coping strategies. This emphasizes the need for future research to validate the results of the study.
Conclusion
A causal model was developed that included coping strategies and their relationships with psychological symptoms. Also, it was found that social support was the strategy that was most likely to reduce emotional concealment, which in turn had the most significant mediating effects on the other disengagement strategies, including the strategies with the most considerable total effects on certain psychological symptoms. This conclusion is based not only on the direct effect that social support had on emotional concealment, but also on the fact that social support was not affected by the presence of the psychological symptoms analyzed in this study. Applying the results to the therapeutic field, it could be inferred that a special focus on improving social skills, and/or searching for social support may have a positive impact on emotional concealment and, as a consequence, on the mental health of those patients who suffer from the symptoms that were described in the present study. Even so, it is noted that the positive effects of social support may not sustain in the long term without complementary interventions, as longitudinal studies have found positive associations between social support and some symptoms.
Data Accessibility Statement
The data that support the findings of this study are openly available at: https://osf.io/rc7b9/
References
- Augusto-Landa J.M., López-Zafra E., Pulido-Martos M. Inteligencia Emocional Percibida y estrategias de afrontamiento al estrés en profesores de enseñanza primaria: propuesta de un modelo explicativo con ecuaciones estructurales (SEM). Revista de Psicología Social, 2011. Vol. 3 (26), pp. 413—425. DOI:10.1174/021347411797361310
- Budge S.L., Adelson J.L., Howard K.A.S. Anxiety and depression in transgender individuals: The roles of transition status, loss, social support, and coping. Journal of Consulting and Clinical Psychology, 2013. Vol. 3 (81), pp. 545—557. DOI:10.1037/ a0031774
- Byrne B.M. Structural Equation Modeling with AMOS / B.M. Byrne (eds). Routledge/Taylor & Francis, Routledge, 2016.
- Calvete E., Corral S., Estévez A. Coping as a Mediator and Moderator Between Intimate Partner Violence and Symptoms of Anxiety and Depression. Violence Against Women, 2008. Vol. 8 (14), pp. 886—904. DOI:10.1177/1077801208320907
- Cano García F.J., Rodríguez Franco L., García Martínez J. Adaptación española del Inventario de Estrategias de Afrontamiento. Actas Españolas de Psiquiatría, 2007. Vol. 1 (35), pp. 29—39.
- Cheung G.W., Rensvold R.B. Evaluating Goodness-of-Fit Indexes for Testing Measurement Invariance. Structural Equation Modeling: A Multidisciplinary Journal, 2002. Vol. 2 (9), pp. 233—255. DOI:10.1207/S15328007SEM0902_5
- Christensen K.A. et al. Habitual reappraisal in context: peer victimization moderates its association with physiological reactivity to social stress. Cognition and Emotion, 2017. Vol. 2 (31), pp. 384—394. DOI:10.1080/02699931.2015.1103701
- Compas B. E. et al. Coping with stress during childhood and adolescence: Problems, progress, and potential in theory and research. Psychological Bulletin, 2001. Vol. 1 (127), pp. 87—127. DOI:10.1037/0033-2909.127.1.87
- Compas B.E. et al. Coping, emotion regulation, and psychopathology in childhood and adolescence: A meta-analysis and narrative review. Psychological Bulletin, 2017. Vol. 9 (143), pp. 939—991. DOI:10.1037/bul0000110
- Connor-Smith J.K. et al. Responses to stress in adolescence: Measurement of coping and involuntary stress responses. Journal of Consulting and Clinical Psychology, 2000. Vol. 6 (68), pp. 976—992. DOI:10.1037/0022-006X.68.6.976
- Connor-Smith J.K., Compas B.E. Coping as a Moderator of Relations Between Reactivity to Interpersonal Stress, Health Status, and Internalizing Problems. Cognitive Therapy and Research, 2004. Vol. 3 (28), pp. 347—368. DOI:10.1023/ B:COTR.0000031806.25021.d5
- Core Team Vienna. R: A language and environment for statistical computing. URL: https://www.R-project.org/ (Accessed 21.10.2021).
- Hinton P., McMurray I., Brownlow C. SPSS Explained 2nd ed. / P. Hinton, I. McMurray, C. Brownlow (eds.). New York: Routledge, 2014. 371 p.
- Hu L., Bentler P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal, 1999. Vol. 1 (6), pp. 1—55. DOI:10.1080/10705519909540118
- Jose P.E., Huntsinger C.S. Moderation and Mediation Effects of Coping by Chinese American and European American Adolescents. The Journal of Genetic Psychology, 2005. Vol. 1 (166), pp. 16—44. DOI:10.3200/GNTP.166.1.16-44
- Kline R.B. Principles and practice of structural equation modeling 4th ed. / R.B. Kline (eds.). New York: The Guilford Press, 2015. 534 p.
- Korkmaz S., Goksuluk D., Zararsiz G. MVN: An R Package for Assessing Multivariate Normality. The R Journal, 2014. Vol. 2 (6), pp. 151—162. DOI:10.32614/ RJ-2014-031
- Kotov R. et al. The Hierarchical Taxonomy of Psychopathology (HiTOP): A dimensional alternative to traditional nosologies. Journal of Abnormal Psychology, 2017. Vol. 4 (126), pp. 454—477. DOI:10.1037/abn0000258
- Lazarus R.S. Coping theory and research: past, present, and future. Psychosomatic Medicine, 1993. Vol. 3 (55), pp. 234—247. DOI:10.1097/00006842-199305000-00002
- Lazarus R.S., Folkman S. Stress, appraisal, and coping / R.S. Lazarus, S. Folkman (eds.). New York: Springer publishing company, 1984. 305 p.
- Lee C. et al. A Closer Look at Self-Esteem, Perceived Social Support, and Coping Strategy: A Prospective Study of Depressive Symptomatology Across the Transition to College. Journal of Social and Clinical Psychology, 2014. Vol. 6 (33), pp. 560—585. DOI:10.1521/jscp.2014.33.6.560
- Leys C. et al. Detecting multivariate outliers: Use a robust variant of the Mahalanobis distance. Journal of Experimental Social Psychology, 2018. (74), pp. 150—156. DOI:10.1016/j.jesp.2017.09.011
- Mardia K.V. Measures of multivariate skewness and kurtosis with applications. Biometrika, 1970. Vol. 3 (57), pp. 519—530. DOI:10.1093/biomet/57.3.519
- Marsh H.W., Hau K.-T., Wen Z. In Search of Golden Rules: Comment on Hypothesis-Testing Approaches to Setting Cutoff Values for Fit Indexes and Dangers in Overgeneralizing Hu and Bentler’s (1999) Findings. Structural Equation Modeling: A Multidisciplinary Journal, 2004. Vol. 3 (11), pp. 320—341. DOI:10.1207/ s15328007sem1103_2
- Ortega A., Brenner S.-O., Leather P. Occupational Stress, Coping and Personality in the Police: An SEM Study. International Journal of Police Science & Management, 2007. Vol. 1 (9), pp. 36—50. DOI:10.1350/ijps.2007.9.1.36
- Park S.-M., Cho S., Moon S.-S. Factors associated with suicidal ideation: Role of emotional and instrumental support. Journal of Psychosomatic Research, 2010. Vol. 4 (69), pp. 389—397. DOI:10.1016/j.jpsychores.2010.03.002
- Prati G., Pietrantoni L. Optimism, Social Support, and Coping Strategies As Factors Contributing to Posttraumatic Growth: A Meta-Analysis. Journal of Loss and Trauma, 2009. Vol. 5 (14), pp. 364—388. DOI:10.1080/15325020902724271
- Preacher K.J., Hayes A.F. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods, 2008. Vol. 3 (40), pp. 879—891. DOI:10.3758/BRM.40.3.879
- Qian X.L., Yarnal C. The role of playfulness in the leisure stress-coping process among emerging adults: an SEM analysis. Leisure/Loisir, 2011. Vol. 2 (35), pp. 191— 209. DOI:10.1080/14927713.2011.578398
- Rankin J.A. et al. Unmet social support needs among college students: Relations between social support discrepancy and depressive and anxiety symptoms. Journal of Counseling Psychology, 2018. Vol. 4 (65), pp. 474—489. DOI:10.1037/cou0000269
- Rosseel Y. lavaan: An R Package for Structural Equation Modeling. Journal of Statistical Software, 2012. Vol. 2 (48), pp. 1—36. DOI:10.18637/jss.v048.i02
- Satorra A., Bentler P.M.A Scaled Difference Chi-Square Test Statistic for Moment Structure Analysis. SSRN Electronic Journal, 2000. Vol. 4 (66), pp. 507—514. DOI:10.2139/ssrn.199064
- Sommer G., Fydrich T. Soziale Unterstützung, Diagnostik, Konzepte, Fragebogen F-SozU / G. Sommer, T. Fydrich (eds.). Tübingen: Deutsche Gesellschaft für Verhaltenstherapie, 1989.
- Sontag L.M., Graber J.A. Coping with perceived peer stress: Gender-specific and common pathways to symptoms of psychopathology. Developmental Psychology, 2010. Vol. 6 (46), pp. 1605—1620. DOI:10.1037/a0020617
- Stat. BA Deutsches Statistisches Bundesamt: Bevölkerung nach Bildungsabschluss in Deutschland [Electronic resource]. Available at: https://www.destatis.de/ DE/Themen/Gesellschaft-Umwelt/Bildung-Forschung-Kultur/Bildungsstand/ Tabellen/bildungsabschluss.html#fussnote-1-104098
- Stine R. An Introduction to Bootstrap Methods. Sociological Methods & Research, 1989. Vol. 2—3 (18), pp. 243—291. DOI:10.1177/0049124189018002003
- Stone L.B. et al. Co-rumination predicts the onset of depressive disorders during adolescence. Journal of Abnormal Psychology, 2011. Vol. 3 (120), pp. 752—757. DOI:10.1037/a0023384
- Suls J., Fletcher B. The relative efficacy of avoidant and nonavoidant coping strategies: A meta-analysis. Health Psychology, 1985. Vol. 3 (4), pp. 249—288. DOI:10.1037/0278-6133.4.3.249
- Tobin D. L. et al. The hierarchical factor structure of the coping strategies inventory. Cognitive Therapy and Research, 1989. Vol. 4 (13), pp. 343—361. DOI:10.1007/ BF01173478
- Tritt K. et al. Kennwerte des Fragebogens ICD-10-Symptom-Rating (ISR). PPmP — Psychotherapie · Psychosomatik · Medizinische Psychologie, 2009. Vol. 02 (59), pp. 409—418. DOI:10.1055/s-0029-1208202
- Troy A.S., Shallcross A.J., Mauss I.B. A Person-by-Situation Approach to Emotion Regulation. Psychological Science, 2013. Vol. 12 (24), pp. 2505—2514. DOI:10.1177/0956797613496434
- Venables W.N., Ripley B.D. Modern Applied Statistics with S / W.N. Venables, B.D. Ripley (eds.). New York, NY: Springer, 2002. 268 p.
- World Health Organization Global Health Estimates 2016: Disease burden by Cause, Age, Sex, by Country and by Region, 2000—2016. Geneva, 2018.
- Yu C.-Y. Evaluating cutoff criteria of model fit indices for latent variable models with binary and continuous outcomes, 2002. 183 p.
- Yung Y.-F., Bentler P.M. Bootstrapping techniques in analysis of mean and covariance structures. In G. Marcoulides, R. Schumacker (eds.) Advanced structural equation modeling: Issues and techniques. East Sussex: Psychology Press, 1996, pp. 195—226.
Information About the Authors
Metrics
Views
Total: 478
Previous month: 12
Current month: 6
Downloads
Total: 236
Previous month: 6
Current month: 2