Research Problem
When analyzing abnormal mental development, it is of particular importance to identify not only patterns common to different types of development, but also specific patterns inherent in a particular type of development (e.g., mental retardation) or even in the development of a particular child. If the solution of the first problem requires the discovery of universal characteristics and mechanisms of development inherent in all types of deviant development, the solution of the second problem is directly related to the concept of “psychological structure of the defect”. Identification of general and specific regularities is essential for qualitative (rather than quantitative) differential diagnostics, as well as, what is especially important, for the design of individually oriented psychological and psychological-pedagogical assistance to children and adolescents with developmental problems. It is the consideration of such regularities and the psychological structure of the defect that makes it possible to determine the principles of interaction with the child, which will contribute to his/her mental development [Lubovskii, 1971; Lubovskii, 1989; Lubovskii, 2016; Lubovskii, 2018; Lubovskii, 2023; Polyakov, 2023; Sevast'yanova, 2020; Slepovich, 2022]. Despite the importance of these categories for helping children and adolescents, they are very rarely used in the practice of psychological diagnosis and correction of developmental deviations [Lubovskii, 2016].
L.S. Vygotsky drew attention to the problem of general regularities of abnormal development [Vygotskii, 2001; Vygotskii, 1983]. For example, as the most general such pattern he noted the violation of interaction with others, which is observed in all types of abnormal development. He also pointed to the hierarchy of disorders, describing the concept of the psychological structure of the defect.
Later, based on the works by L.S. Vygotsky, V.I. Lubovsky described a number of other general regularities of abnormal development on the basis of empirical studies available in special psychology [5-9]. These include violations of verbal mediation in the formation of new connections, a slower rate of reception and processing of sensory information and a smaller volume of information captured and stored in memory, defects in the development of arbitrary movements, increased fatigue, and a slower rate of mental development.
At the same time, V.I. Lubovsky, I.A. Korobeinikov and S.M. Valyavko point out the importance of identifying specific patterns of abnormal development that reveal the qualitative features of a particular type of development [Lubovskii, 2016; Lubovskii, 2018]. This problem has been more or less successfully solved in relation to certain categories of children, relying on the concept of the psychological structure of the defect. Thus, defect structures have been described in mental retardation, learning disabilities, early childhood autism, visual and hearing impairments [1; 4—9; 15; 16].
Appeal to the concept of psychological structure of defect as a tool of psychological diagnosis encourages us to see deviations in development not as a series of symptoms, but as having a certain hierarchy. According to L.S. Vygotsky, the primary defect is directly related to organic damage or dysfunction in this hierarchy [Vygotskii, 2001]. For example, damage to the cochlea of the auditory analyzer is directly related to auditory perception disorders. The second-order defect is related to the primary defect (in this example, developmental disorders of oral speech). However, this connection is already less rigid and depends on various social conditions. The same pattern applies on the formation of defects of the third and so on orders — the higher the order of the defect, the less it is predetermined by biological factors and the more it depends on the interaction of the child with others. As V.V. Lebedinsky, high-order defects are less rigidly related to a particular type of deviant development and are less specific for it [Lebedinskii, 2003].
We should pay attention to the fact that another concept of the psychological structure of a defect is of particular importance for solving the problem of providing practical help to a child. It is the concept that reveals the specifics and mechanisms of development of a particular child [Lubovskii, 2016; Lubovskii, 2018; Polyakov, 2023; Slepovich, 2022]. However, what does this concept consist in? Should we adjust our ideas about the psychological structure of the defect, considered in relation to an individual child, rather than a clinical diagnosis? What opportunities does such an understanding of the term provide us for solving practical problems?
Nuclear disorder in the structure of the defect
We understand the psychological structure of the defect as reflecting deviations in the formation of the psyche of an individual child. It allows us to select specific ways of assistance taking into account the unique specifics of his/her development [Lubovskii, 2016; Sevast'yanova, 2020]. For example, V.I. Lubovsky notes that in some cases a visually impaired child can rely primarily on touch and a child, defined as blind, can use residual visual perception [Lubovskii, 1971]. In this context, the author speaks of a special way of interacting with the environment. In a child with ADHD in one case behavioral problems are associated with immaturity of mechanisms of processing kinesthetic information, and in another case — with problems of formation of child-parent relations and immaturity of social motives. It is important for us to understand that the psychological characteristics of interaction with the world and the characteristics of mental development can be quite different in children and adolescents with the same clinical diagnosis. Undoubtedly, this is of fundamental importance for determining the strategy and tactics of psychological and pedagogical assistance to a particular child. In the future we will use the latter meaning of the term “psychological structure of the defect”, i.e., we will apply it to the analysis of the development of a particular child rather than a clinically defined type of development.
In this context, it is important to draw attention to another problem in defining the psychological structure of a defect. It concerns the term “primary defect”, which, as already noted, is directly related to organic impairment [Vygotskii, 2001]. However, in practice, it is not always possible to determine the organic damage. This is especially true for mild, borderline, states and types of abnormal development. In addition, many variants of abnormal development are not based on organic damage at all, but are caused exclusively by social factors or are caused by their combined effect (e.g., learning disabilities of psychogenic or somatogenic origin). In these cases, we believe it is legitimate to speak not so much of a primary defect as of a nuclear disorder of the psyche underlying the whole variety of individual manifestations of abnormal development of a particular child [Slepovich, 2022]. It is often impossible to determine the relationship of a nuclear defect to organic or functional brain damage.
Identification of a nuclear defect during psychodiagnostic examination involves qualitative analysis of the characteristics of the child’s interaction with other people and ways of solving various tasks. The nuclear defect reveals itself in most of the child’s actions or underlies them. For example, the weakness of analysis of sensually perceived characteristics of the object can be manifested in a child of 7 years old in the problems of mastering reading (slow reading in syllables), mastering the image of the letter and difficulties in neat writing, inability to put together a pattern of Koos cubes, to carry out phonemic analysis of a word, to identify the elements of a complex movement (insufficient differentiation of movements) or correct posture (for example, to hold a pen correctly), and many others. Secondary to a nuclear defect, there may be difficulties in reading comprehension, problems of speech communication, interaction with peers in outdoor games, arbitrary regulation, etc. Determining in this case the initial organic disorder is extremely difficult, and does not make much sense. At the same time, the allocation of the nuclear defect allows us to organize psychological and pedagogical assistance in accordance with the peculiarities of the child’s development. It can be aimed either at overcoming the nuclear defect, or at bypassing it and using the preserved sides of the psyche, or at changing the attitude to it, or at the combined use of the first, second and third, depending on the specifics of the developmental abnormality. Such understanding of the structure of the defect once again emphasizes the importance of quality psychological diagnostics, based not so much on the specialist’s assessment of the speed and performance of test tasks, but on a meaningful analysis of how the child acts and combining the results of such analysis into a holistic model.
Objective type of response to the defect
The second aspect of the revision of the concept of the “psychological structure of the defect”, related to its use in the in-depth psychological diagnosis of abnormal child development, touches on possible ways of the formation of higher order defects. L.S. Vygotsky noted the importance of our understanding not only the initial problem that the child faced in his development, but also how the personality reacts to it [Vygotskii, 2001]. It is important that such a reaction is not predetermined by the primary defect itself, but is related to the nature of social interaction. L.S. Vygotsky uses the concept of hypercompensation to describe the possible response of the personality to the defect. Later, for special psychology, the idea of the formation of defects of the second, third, etc. order became commonplace, their appearance began to be taken for granted and lost the character of a scientificproblem. However, do high-order defects really arise “automatically”? What are the possible reactions of an individual to a nuclear defect? Is it possible to construct some typology of such reactions? What are the conditions of formation and change of the reaction type? The answers to these questions are extremely important for the psychological and pedagogical support of children and adolescents with developmental disabilities, since the nuclear defect itself is only one of the characteristics of the personality, and its socialization and quality of life are ultimately determined by the way it reacts to this characteristic.
We believe that there are two types of personality response to the defect (developmental problem) — objective and subjective.
The objective type of response is changes in the work of the psyche (functions, behavior, regulatory mechanisms, motivation, connections between components of the psyche) under the influence of a lower-order defect. We can distinguish three variants of such changes:
(a) strengthening of characteristics of some functions under the influence of others: increased motor activity with reduced kinesthetic sensitivity; development of hypertrophied interest in inanimate objects, fields (e.g., astronomy) with problems of social interaction; advanced development of formal-logical thinking with lack of ability to empathize; strengthening of mechanical memory with difficulties of social adaptation, etc.;
(b) weakening of the characteristics of some functions under the influence of others: slowing down of the speed of recognition of objects in the process of visual perception in hearing-impaired people; decreased learning motivation in systemic speech disorders or difficulties in visual analysis of objects; immaturity of arbitrary control of actions against a background of increased emotional arousal or distortion of relationships with other people in some behavioral disorders, etc.;
(c) changes in the ratio of mental functions (their hierarchical relations) that is not typical of age: strengthening of the role of mechanical memory with inability to comprehend the studied material at school age; dominance of affective regulation of behavior over verbal regulation; dependence of emotions and behavior on the perceived field rather than on one’s own goals and semantic regulation, starting from the senior preschool age, etc.).
In general, the objective type of response to the defect determines changes in the person’s ways of acting. Such changes are designed to help socialize and adapt to the world around them. Thus, for example, difficulties in reading comprehension in dyslexia can lead to excessive concentration of the child on the external side of reading, on decoding graphemes into phonemes. Problems in mastering the motor side of speech may lead to the child’s refusal to use active speech in communicating with others and the predominance of nonverbal communication. At the same time, a change in the mode of action is not always negative in terms of mental development. For example, deficiencies of mechanical memory can provoke the use of methods of comprehension and logical organization of information when solving tasks for memorization. Difficulties in the automation of actions and serial organization of movements can contribute to the emergence of a pronounced desire to arbitrarily control them. Thus, the objective type of response, changing the ways of action, can both generate new problems in the development, socialization and social adaptation (higher-order defects) of an individual, and contribute to overcoming the nuclear defect and previously formed limitations in the functioning of the psyche, the emergence of qualitatively new ways of solving vital tasks.
Subjective type of response to the defect
The subjective type of response is a person’s experience of a defect (developmental problem). It should be correlated with such a concept as the internal picture of the defect, which is now increasingly used by clinical and child abnormal psychologists [Gaidukevich, 2019; Sevast'yanova, 2020; Tikhonova, 2019]. This concept is compared with the concept of the internal picture of the disease, but it is not identical to it. For example, it is rather difficult (at least in some cases) to talk about the sensory component of the internal picture of the defect, since we are not talking about a disease, as a rule, which changes a person’s self-perception, but about the background state with which a person lives constantly. The attitude to one’s own defect requires the child to reach a certain level of self-consciousness development. In this regard, based on our practical experience, we propose to distinguish three components in the structure of the subjective type of personal response to the defect (and possibly in the structure of the internal picture of the defect) — attitude to the defect, emotional-sensual and behavioral components. Let us consider them in detail.
1. Attitude to the defect can be represented through such categories as identification with the defect and awareness of the defect. Identification with the defect is its experience as an integral part or characteristic of one’s own Self. Identification with the defect is related to, but not equal to, acceptance of the defect, since acceptance implies a conscious relationship to one’s own specificity. At the same time, identification can also take place at an unconscious level, just as it can in relation to normal human characteristics, which are expressed in our expectations, self-perception, habitual reactions to different situations, etc. These characteristics, however, are not the subject of reflection. At the same time, they are not the subject of reflexive attitude. Against this background, we may perceive some of our sensations, feelings, states, reactions, achievements (or inability to cope with something) as alien to us.
The second characteristic of the attitude to the defect is its awareness, i.e. the representation of the characteristics or manifestations of abnormal development for the person himself in a sign and symbolic (not necessarily verbal) form, expressing their connection with his Self and life. The latter aspect is most clearly manifested in the intertwining of representations of the defect in the symbolism of autobiographical memories and narratives, as well as expectations about the future. Working with them, we can change the individual’s attitude to his or her own defect in the course of psychological help [Nurkova, 2022; Polyakov, 2022; 20; 21]. Awareness of one’s own defect allows him or her to connect it with one’s own Self and to realize how it affects the agent’s actions and changes his or her life.
Combining two characteristics of attitude towards the defect — identification with it and its awareness, we get four possible types of attitude (presented in the table).
The first type is naive or natural, in which there is no identification with the defect and its awareness. In this case, subjectively the defect of mental work does not exist for the child or adolescent. It is not represented in his experience. The second type is the avoidant type. In this case, identification with the defect is observed, but it is presented in the experience only as a difficulty in any kind of activity (speech communication, solving some learning tasks, etc.). There is no realization of the content of these difficulties. The problem is not verbalized by the child. Its existence in subjective terms can be judged only on the basis of tacit avoidance of those types of activity in the construction of which defective mental functions play a significant role. Thus, for example, very often children who have difficulties in constructing a speech utterance begin to avoid speech communication. The third type — defensive — represents the awareness of the problem (a defect in the work of the psyche) against the background of experiencing it as something alien. For example, a child (adolescent) may realize that he or she occasionally experiences uncontrollable rage, but views it as an external force in relation to his or her Self. The child may realize the uncontrollable and chaotic nature of his/her external activity (difficulties in arbitrary control), but not consider it possible to somehow cope with this problem, as it is caused by some external reasons. In this type of attitude to the defect, there may be a variety of defensive reactions associated with the experience of one’s own otherness or failure — withdrawal into oneself, auto-aggression, blaming others and experiencing the injustice of their actions in one’s address, attempts to hide the problem. They can be accompanied by emotions of shame, anxiety, anger, despair, etc. The fourth type — constructive — involves realizing the peculiarities in the work of the psyche and accepting them as one’s own. The defect is experienced as part of one’s own personality and is included in the structure of identity. At the same time, it is no longer perceived as a defect, but rather realized as a feature of the personality. This type of attitude allows one to recognize the existence of certain problems and learn to intentionally use constructive ways of coping with them. This may include seeking help from other people, accepting one’s own limitations, discovering and using available ways of solving life’s problems by relying on one’s abilities (compensation), turning one’s “weaknesses” into “strengths” by rethinking them (e.g., anxiety may motivate one to be attentive), and so on. We believe that the change in the types of attitude to the defect is related to the level of mental development of the child and can occur in the direction from the first type to the fourth in the process of psychological assistance.
2. The second component in the structure of response to the defect — emotional-sensual — is changes in the subjective significance of elements of experience and, accordingly, emotional sensitivity and reactions under the influence of the defect. Such changes can be expressed in the experience of emotional discomfort or fears about the sounds of other people’s voices, emotional tension in the process of communication, perceived as excessive and unbearable, intolerance of one’s own tension when solving difficult tasks, exclusion from the realized repertoire of emotions of weak in intensity experiences and the discovery of only strong ones approaching the state of affect (because of which they acquire an explosive character), the experience of the usual requirements of an adult as insulting and humiliating. In the context of psychological practice of work with children and adolescents, their rethinking of their sensual-emotional experience through its awareness and expression by means of sign and symbolic forms (for example, verbalization of shades and degree of expression of emotions, establishing the connection of their own experiences with certain actions and situations) acquires special value.
3. The third component — behavioral — represents changes in the direction of behavior and actions in connection with the agent’s experience of his own defect (problem). The behavioral component is a reaction to the inability to perform some action or difficulties arising in this case. It can be expressed in avoidance of a difficult action, situations (communication with other people, visiting places where subjectively experienced problems may arise (e.g., school)); compensatory immersion in activities in which the child feels well-off, in order not to be involved in uncomfortable situations; hypercompensatory manifestation of efforts aimed at coping with the problem (cannot agree with another person and tries to force him/her; chronically lacks attention from an adult and shows excessive and indiscriminate “clinginess”; cannot memorize material and repeats it many times, etc.); dependent behavior, in which the other is perceived as a source of solving the child’s problems and satisfying his or her needs, etc.). It is important to note that the child’s behavior and actions, due to their orientation, can both support the existing nuclear defect and contribute to its overcoming through the formation of insufficiently mature functions, the use of compensatory mechanisms or coping strategies. It is extremely important to take this point into account when providing psychological help to a child and to promote the formation of an adequate orientation of actions that will help to cope with the existing difficulties.
Table. Types of agent’s attitude to his/her own developmental defect
|
Identification with the defect \ Awareness of the defect |
Is not aware |
Is aware |
|
Does not identify |
(1) Naive (natural) type |
(3) Defensive type |
|
Identifies |
(2) Avoidant type |
(4) Constructive type |
The principle of cyclicality
Generalizing the ideas about objective and subjective types of response to the defect, it is necessary to introduce the principle of cyclicality formation of the defect structure. This principle suggests that the very reaction to a nuclear defect is fundamentally important for fixing and possibly even strengthening the original problem or for overcoming it in the broader context of mental development and socialization of an individual by changing the ways and direction of the agent’s actions. Reaction to a defect can form cycles of two types. The first, the dysfunctional cycle, triggers a mechanism for maintaining or reinforcing the nuclear defect and generating new defects of higher-order mental functioning. Such changes create and aggravate problems of interaction with the surrounding world and the development of the psyche as a whole, eventually leading to the aggravation of the original problem. Similarly, maintenance processes or cycles are described in cognitive behavioral therapy (see, for example: [Uait, 2010; Polyakov, 2022a]). The difference is that the latter reflect processes of maintaining mainly the subjectively experienced problem rather than abnormalities of mental functioning and development. The second — evolutionary cycle — provides the mechanism of normal mental development, using the nuclear defect as an individual feature, a characteristic that must be reckoned with, that can be used in designing ways of interacting with the world, that can be changed and compensated for by available means and methods. Productive use of the nuclear defect or its compensation, successes in the processes of socialization and social adaptation in turn contribute to a change in the agent’s attitude to the nuclear defect, its better understanding and discovery of new opportunities to cope with it.
In general, it can be stated that when providing psychological assistance to a child with developmental disabilities, one should work on changing the attitude to the nuclear defect, rethinking the emotional and sensory component of subjective response and developing constructive forms of meaningful activity that contribute to overcoming the existing difficulties, taking into account the objective changes in the psyche that occur under the influence of the nuclear defect. Attention should be paid both to the ways of reacting to the defect and to its orientation, expressed in the actions of the agent. It is important to distinguish changes in the child’s activity as manifestations of the nuclear defect from manifestations of the personality’s reaction to it. Thus, a lag in development or the absence of expressive movements and expressive gestures in the child’s repertoire of social interaction can be both a manifestation of the initial damage to the mechanism of movement construction (for example, in mental retardation) and a secondary reaction to difficulties in communication and the associated experience of anxiety.
For clarity, we have presented the described psychological structure of the defect in application to the analysis of abnormal development of a particular child in the form of a scheme (Fig.).
Conclusion
Thus, analyzing the concept of psychological structure of the defect, its applicability to the disclosure of individual features of abnormal development of the child is revealed. Its application allows us to determine the direction and strategy of psychological help, as well as to identify specific educational needs. This concept forces not just to discover the symptoms of abnormal development, but to investigate the dynamics of their formation and hierarchical relations between them.
Under the psychological structure of the defect in this article it is proposed to understand the totality of nuclear violations of the psyche, setting the whole range of private manifestations of abnormal development of an individual, as well as the agent’s reaction to them.
The formation of higher-order defects is associated with the peculiarities of the child’s social interaction, which allows us to talk about different types of personality response to defects in the work of their own psyche. Objective and subjective types of response are singled out. The first reveals objective changes in the psyche under the influence of lower-order defects and determines changes in the individual’s ways of action. The subjective type of reaction reveals the experiences of the individual about the defect and sets the direction of actions and behavior in relation to it. It determines the psychological content of the experience related to the problems of functioning of the child’s psyche.
The agent’s reaction to the defect can trigger cycles of two types: a dysfunctional cycle, which supports the existence of the nuclear defect and generates higher-order defects, and an evolutionary cycle, which provides the mechanism of coping with the original violation. Working on changing the ways and direction of response to the nuclear defect is one of the key tasks of psychological assistance to a child with developmental disabilities, allowing to take into account its individual specificity.
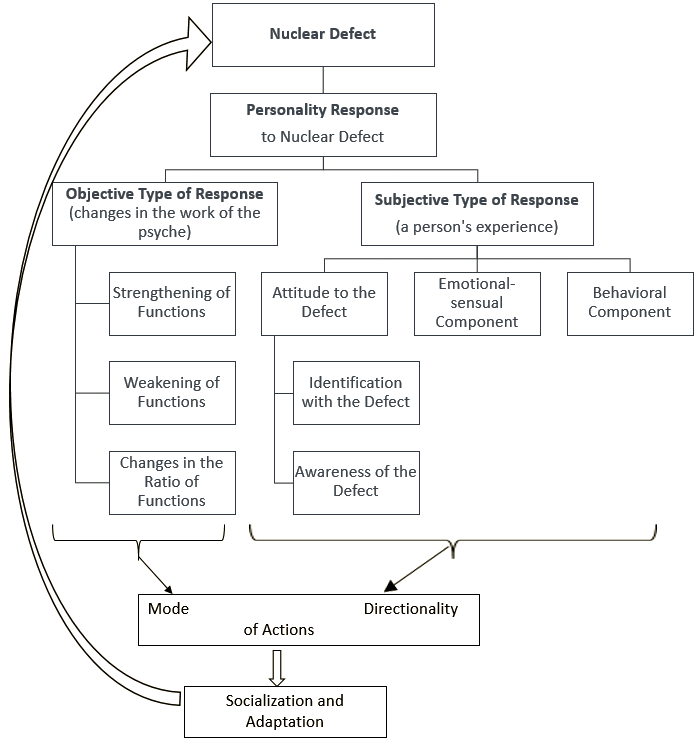
Fig. Psychological structure of the defect
When providing psychological help, in some cases it is advisable to focus on overcoming the nuclear defect, in other cases — on working with the reaction of the personality to it, in third cases — on the first and the second. This depends on whether the nuclear defect is amenable to psychological correction, the age of its occurrence and the age at which help is provided, the specific ways in which the personality responds to it. In addition, the psychological structure of the defect, unique for a particular child, determines the logic of interaction between the psychologist and related specialists in the design and implementation of the correctional program.