1. Introduction
The number of children being diagnosed with Autism Spectrum Disorder (ASD) has increased in recent years. About 1 in 54 children has been identified with ASD in the United States [3]. And it was reported a similar prevalence of ASD in China to the West [31]. ASD is a life-long pervasive developmental disorder and will take lifelong challenges to individuals [10]. As such, a child diagnosed with ASD may represent a constant source of stress on the family unit [11] due to the enormous care and the psychological burden. Family functioning is an important source of support for the family [14]. So strengthening family functioning is key for the support of families raising a child with ASD. A useful strategy to support these families in counseling practice is the concept of Circumplex Model.
1.1. Circumplex Model — interaction between family cohesion and adaptability
Olson et al. proposed the Circumplex Model in the late 1970s and indicated a balanced level of both cohesion and adaptability was the most functional to family development [24]. Both family cohesion and adaptability reflect important interactions in a family, which are determinants of family “health”.
Family cohesion refers to the emotional bonding members have with one another and the degree of individual autonomy a person experiences in the family system, while family adaptability was defined as the ability of a marital/family system to change its power structure, role relationships, and relationship rules in response to situational and developmental stress [24]. According to the Circumplex Model, the combinations of the four levels of family cohesion (i.e., disengaged, separated, connected, and enmeshed) and the four levels of family adaptability (i.e., rigid, structured, flexible, and chaotic) give a total of sixteen types of family systems: four types have unbalanced scores (very high or very low scores) on both cohesion and adaptability and are considered “extreme”, eight types that are balanced in one dimension and unbalanced in the other dimension are considered “mid-range”, and four types in the center area are considered “balanced”. Olson, Sprenkle and Russell [24] suggested that the optimum level was the central area of the Circumplex Model, namely the balanced families, which was seen as most functional to individual and family development and families were better able to adapt to the stresses of caring for a child with ASD. However, the extreme families represent the different types of dysfunctional family, being the most problematic in terms of global functioning [13]. In the first case, highly enmeshed families (i.e., the most cohesive family type) are overly involved in and protective of their children's lives and may not promote the growth and independence of the child. At the opposite pole, disengaged families (i.e., the least cohesive family type) have rigid boundaries between family roles and the child would be free to develop independence but may not feel loved and protected [1]. Looking at the size of adaptability, the rigid family (i.e., with lower level of family adaptability) appears to be characterized by high levels of emotional closure and inadequate flexibility, rules perceived as inviolable, and limited communication to structural models that make difficult an exchange based on reciprocity [13], while chaotic families (i.e., with higher level of family adaptability) are characterized by unstable and inconsistent change [1]. Finally, the mid-range families can be characterized by the combination of reduced flexibility and good cohesion, or vice versa [13], and are likely to transition to the balanced family to achieve the optimal allocation of family functioning [6, p. 36].
There have been few studies that gathered data about family cohesion and adaptability in families of children with ASD, and found that parents of children with ASD suffered from more psychopathology and less dyadic consensus, and as a result perceived less marital satisfaction, emotional expression, and family cohesion and adaptability [9; 11]. Lin et al. [18] reported Taiwanese mothers of adolescents and adults with ASD showed lower levels of family cohesion and adaptability than did the mothers in the U.S. Contrary to this finding, Rodrigue, Morgan, and Geffken [27] reported that parents of children with ASD had higher level of family cohesion and lower level of family adaptability. Given these discrepant findings concerning the level of family cohesion and adaptability in families of children with ASD, together with the importance of family functioning since poorer functioning in families predict poorer levels of functioning in the child with ASD [30], there is a need for further research addressing this issue in different regions. The current study attempted to identify family cohesion and adaptability in Chinese families of children with ASD.
1.2. Factors influencing cohesion and adaptability in families raising a child with ASD
Several factors have been identified for affecting family cohesion and adaptability, such as the characteristics of child, caregiver, and family. For example, Li [17] found that the lower functional levels of children with ASD correlated with greater psychological pressure experienced by their caregivers. Higgins, Bailey, and Pearce [11] highlighted characteristics of children with ASD (such as low social competency and persistency) and the behavioural manifestation of these tendencies affected family functioning in families with a child with ASD. Children's functional level (severity of impairment) is therefore one of the factors influencing family cohesion and adaptability.
In addition to personal characteristics of children, some researchers pointed out that also the personalities of caregivers affected family cohesion [28]. Caregivers of children with ASD tend to have depression, anxiety, obsession-compulsion, interpersonal sensitivity, hostility, schizoid trait, paranoia, and schizophrenia [9]. However, they may also demonstrate positive outcomes as one survey reported half of families believed the arrival of children with ASD had a positive impact on the relationship between couples [19]. Xue, Ooh, and Magiati [34] also found higher positive meanings in Singaporean families raising children with ASD. In other words, resilience in those families was found, which is of great significance for the enhancement of family cohesion and adaptability.
Besides, family functioning was also affected by the family's socioeconomic status [38, p. 14]. Caregivers with lower socioeconomic status were more likely to suffer from stress and mental health problems due to difficult life events such as not being able to pay their bills, losing their jobs, moving frequently, and worrying about money [20]. Regular employment contributed significantly to reduce caregivers' distress and enhance their well-being [21], while families raising a child with ASD had serious negative career impacts due to the need to take care of children [35]. As a result, the growth of negative emotions may lead to the decrease of family cohesion and adaptability.
It is evident that there are many factors that influence family cohesion and adaptability. However, it would be useful to know more about the predictors for the counseling practice with families raising a child with ASD.
1.3. The purpose of the current study
The aim of this study was to explore the perception that Chinese caregivers of children with ASD have of their family cohesion and adaptability and to examine its influencing factors. Findings of the study may add some evidence for understanding of these theoretical concepts and various relationships. Furthermore it can help us to understand better the needs of the family members and to plan a more effective professional support for these families.
The following research questions were examined in the current study:
• What is the level of family cohesion and adaptability in Chinese caregivers of children with ASD according to the Cir- cumplex Model?
• What factors relating to the caregivers of children with ASD can significantly predict the level of family cohesion and adaptability?
2. Methods
2.1. Participants and procedure
Participants parenting a child with ASD less than 18 years old were recruited through special education schools in Sichuan province of China. An informational letter introducing the purpose of this survey and explaining the anonymity and confidentiality of the data was sent to the caregivers of children with ASD. All the participants gave their informed consent, and then were asked to fill in the questionnaires on behalf of the family. This study received institutional approval of Leshan Normal University in China and complied with ethical guidelines. Finally a sample of 190 caregivers of children with ASD was created, and 168 caregivers completed and returned back their questionnaires (a response rate of 88.42%). The respondents included in this study had the following characteristics:
• A total of 144 (86.20%) caregivers were married or living with a partner, the remaining 24 (13.80%) were divorced, separated, or widowed;
• 77 (46.10%) were unemployed, 61 (36.50%) had full time jobs, 16 (9.60%) had part time jobs, and 13 (7.80%) were looking for jobs;
• 48 (28.60%) had received a primary school degree, 32 (19.00%) finished junior school, 28 (16.70%) finished senior high school, 28 (16.70%) finished junior college, and 32 (19.00%) had bachelor or above degree;
• 86 (51.20%) lived in cities, 34 (20.20%) lived in towns, and 48 (28.60%) lived in villages;
• 121 (72.00%) had medium or high income (more than 2000 RMB per month), while 47 (28.00%) had low income (below 2000 RMB per month).
• In terms of children's characteristics, 112 (67.10%) were boys and 55 (32.90%) were
girls; their mean age was 9.73 (SD=2.95); 27 (16.20%) were high functionality level, 61 (36.50%) were medium, 67 (40.01%) were low, and 12 (7.20%) were very low.
A brief demographic questionnaire including child's gender, age, and functional level, caregiver's marital status, educational level, employment status, place of residence, and monthly income were surveyed first.
Then, Chinese version of Family Adaptability and Cohesion Evaluation Scales (FACES II-CV) were used to measure family cohesion and adaptability. These scales were developed by Olson et al. in 1982 and translated by Phillips et al. in 1991. This 30-item self-report questionnaire assesses family functioning by measuring family cohesion (16 items) and family adaptability (14 items). It uses a 5-point Likert scale with the poles “almost never” to “almost always”. Higher scores on family cohesion indicated more connected families and higher scores on family adaptability indicated more flexible families. Family cohesion consists of four levels: disengaged (total score<55.90), separated (total score between 55.90 and 63.90), connected (total score between 64.00 and 71.90), and enmeshed (total score>71.90), and family adaptability also consists of four levels: rigid (total score<44.70), structured (total score between 44.70 and 50.90), flexible (total score between 51.00 and 57.10), and chaotic (total score>57.10). The original scale includes the subject's perception of actual conditions in the family and of ideal family conditions. In this study, the respondents were only required to reflect on the actual conditions.
The FACES II-CV was reported to be a reliable and valid measure, in which the test- retest reliability for Cohesion and Adaptability were 0.84 and 0.91, and the coefficient of internal consistency were 0.85 and 0.73 [25]. In the current study, the Cronbach alpha coefficients of Cohesion and Adaptability were 0.82 and 0.85, and the Cronbach alpha coefficients of the FACES II-CV was 0.91. It lent evidence that the scale was measured in a reliable way.
Statistical analyses were performed using SPSS 18.0 software. Descriptive statistics were used to describe demographic characteristics of the caregivers and children, and caregiver's family cohesion and adaptability. T-test was conducted for the score comparison of family cohesion and adaptability between child's genders, while one-way ANOVA was conducted for scores comparison among child's ages, functional levels, caregiver's marital status, educational levels, employment status, places of residence, and monthly income (items with more than two subcategories). In cases when significant differences in the scores according to one-way ANOVA analysis were found, LSD method would be used for post-hoc comparisons. Multiple linear regression analysis was performed to verify the predictors of family cohesion and adaptability. Statistical significance was set at p- value<0.05 in this study. The reliability of the scales was determined by measuring the Cronbach alpha coefficients.
3. Results
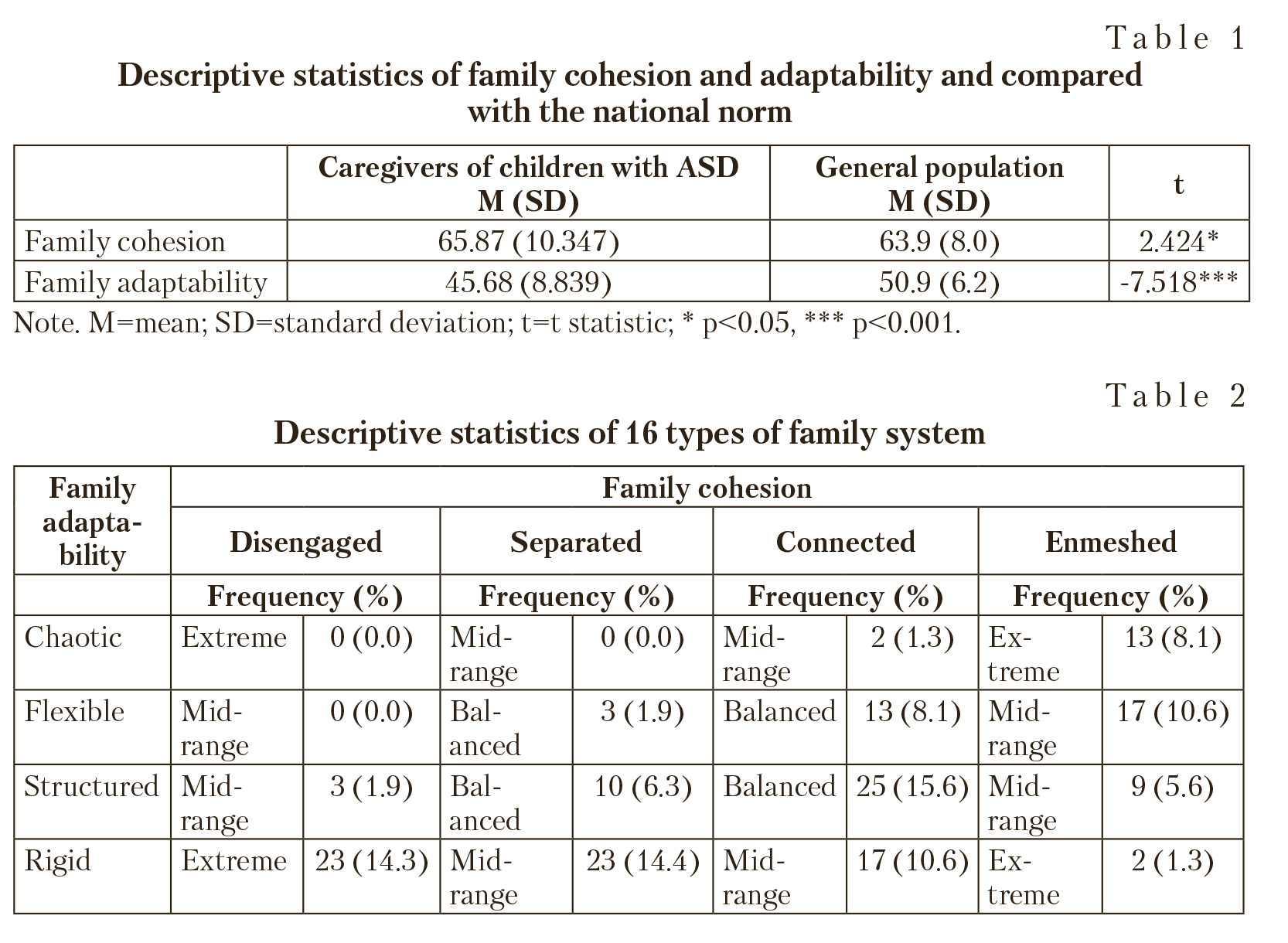
3.1. Family cohesion and adaptability in caregivers raising a child with ASD Descriptive statistics for family cohesion and adaptability were reported in Table 1. It shows that the mean scores of family cohesion and adaptability of caregivers of children with ASD were 65.87 (SD=10.347) and 45.68 (SD=8.839), respectively. When compared to the national norm [6, p. 15], it was found that the score of family cohesion was significantly higher (p<0.05), while the score of family adaptability was significantly lower (p<0.001).
According to the Circumplex Model, the family types of caregivers of children with ASD were mostly “structurally connected” in this study, accounting for 15.6%. Moreover, 44.4% families were mid-range type, 31.9% were balanced type, and 23.7% were extreme type. See Table 2.
3.2. Differences of family cohesion and family adaptability in demographic variables
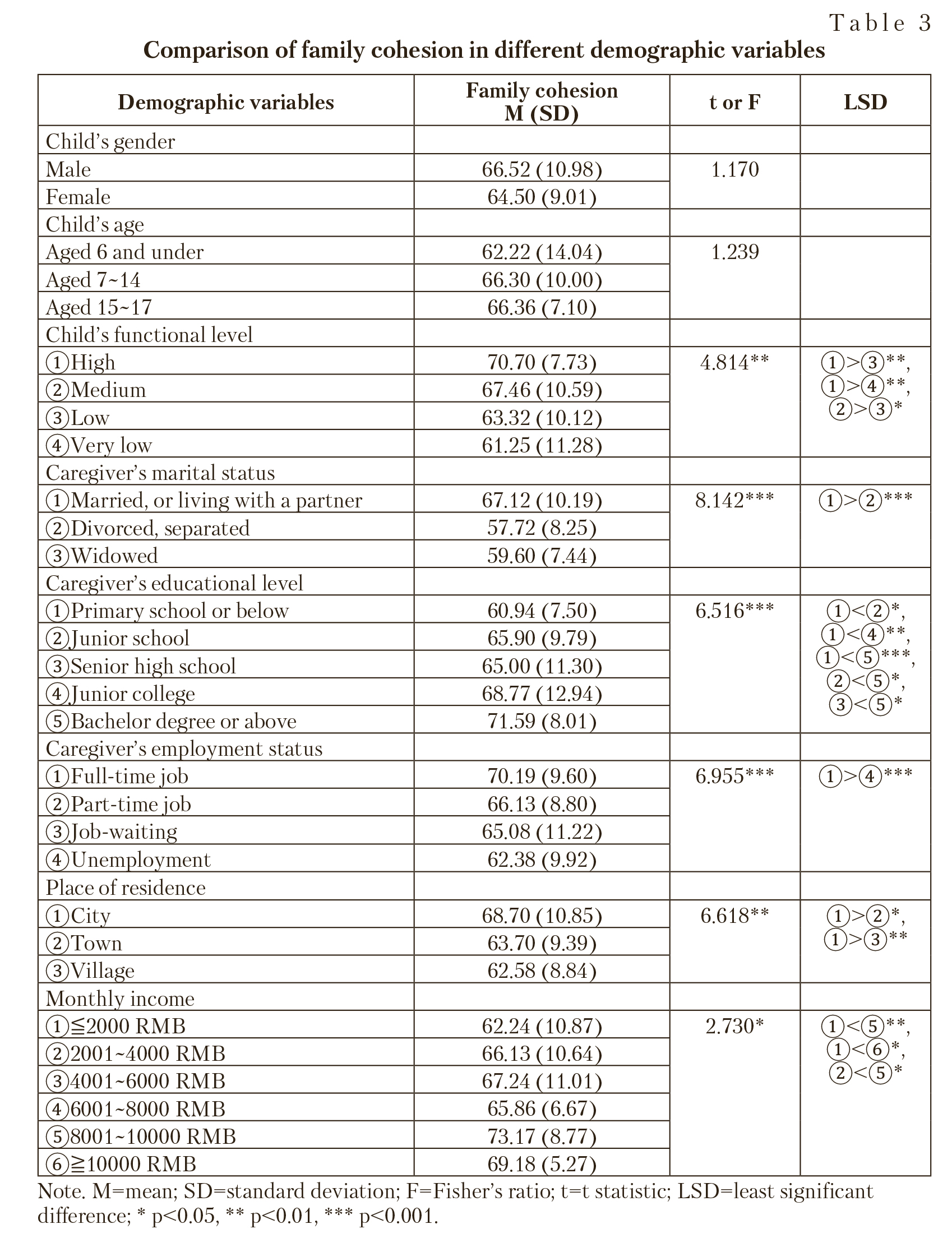
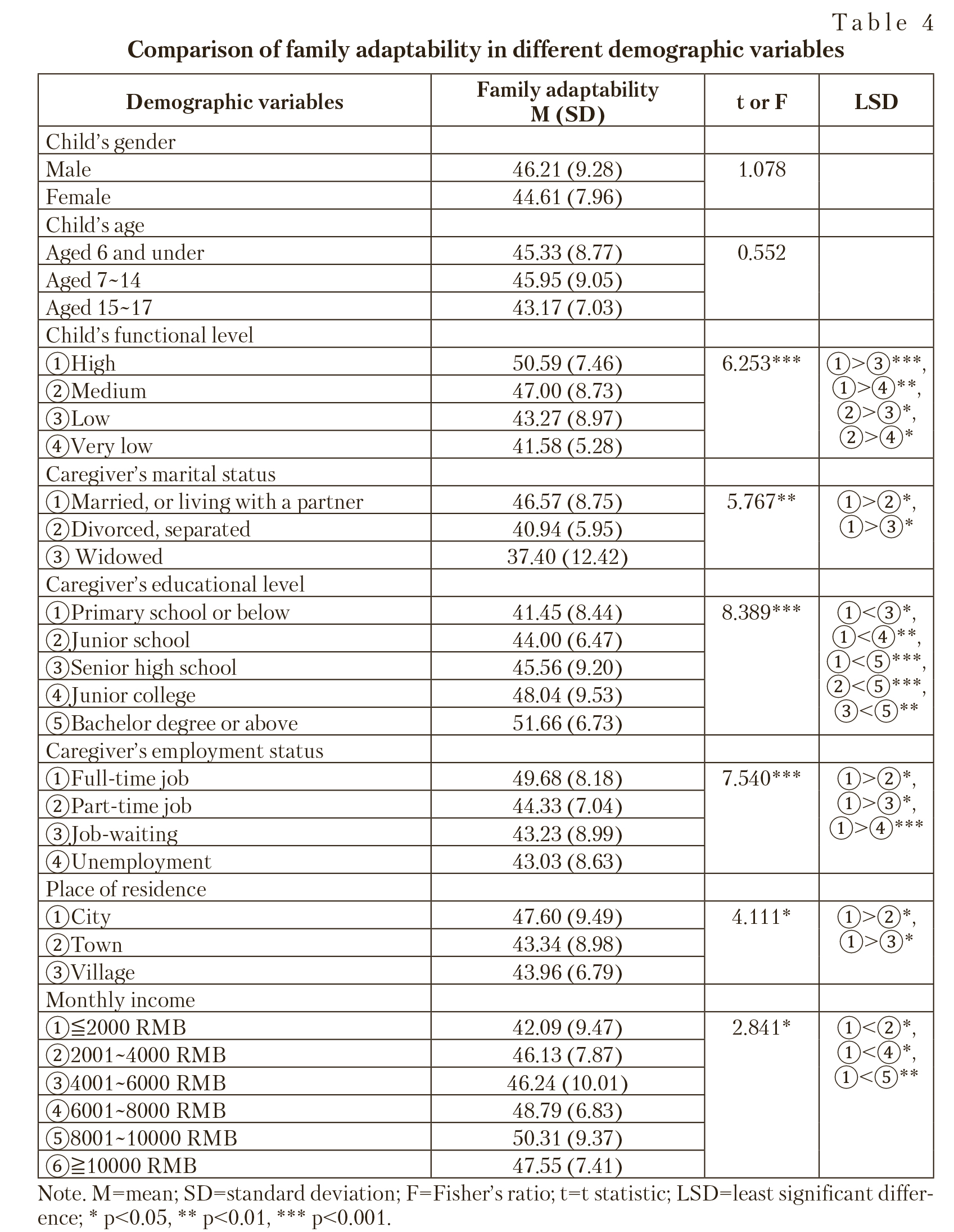
In this study we compared the scores of family cohesion and family adaptability with different demographic variables respectively and found that there were significant differences in the scores of family cohesion and adaptability depending on the child's functional level, caregiver's marital status, employment status, educational level, place of residence and family monthly income (p<0.05). However, there were no significant differences in the scores of cohesion and adaptability in relation to child's gender and age (p>0.05). See Table 3 and Table 4.
3.3. Predictive power of demographic variables on family cohesion and adaptability
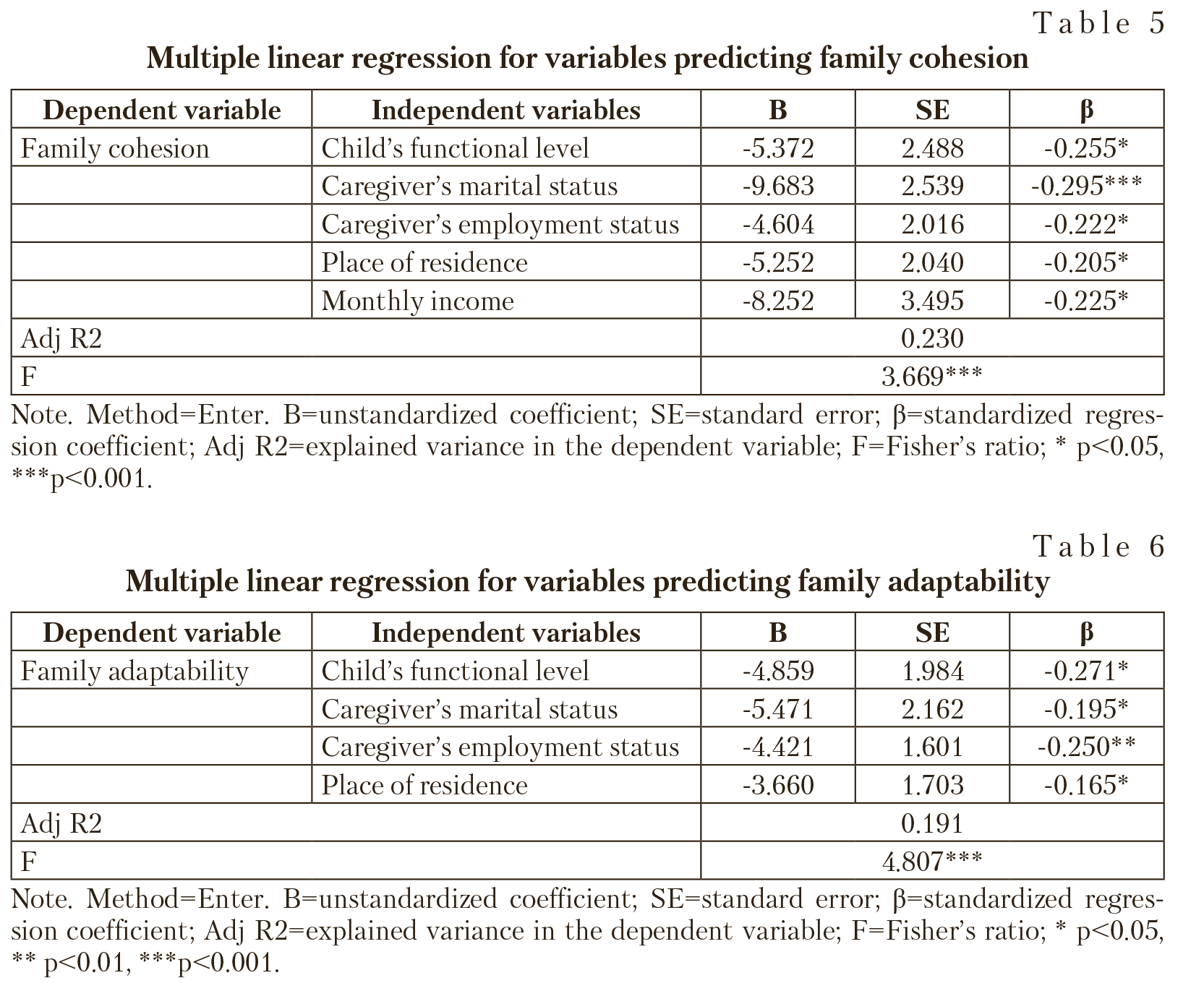
Multiple linear regression analyses were performed in this study on family cohesion and adaptability scores as dependent vari-
ables respectively, demographic variables with significant differences (including child's functional level, caregiver's marital status, educational level, employment status, place of residence, and monthly income) as independent variables, in which classification demographic variables had been set as dummy variables. As presented in Table 5 and Table 6, child's functional level, caregiver's marital status, employment status, place of residence, and monthly income all had significant predictive power to family cohesion (p<0.05), and the child's functional level, caregiver's marital status, employment status, place of residence all had significant predictive power to family adaptability (p<0.05). For more details about the interpretation of the relationships between dependent and independent variables see next section.
4. Discussion
4.1. Cohesion and adaptability
in caregivers raising a child with ASD
In this study, family cohesion perceived by Chinese caregivers of children with ASD was at a higher level as compared to the general population, while their adaptability was at a lower level. It suggests family members of children with ASD were more emotion-
ally connected with each other, but had lower adaptability and resilience while facing difficulties. The result is consistent with the finding of Rodrigue et al. [27], but inconsistent with some previous studies reporting caregivers of children with ASD have lower levels of cohesion and adaptability [9; 11; 34; 38, p. 27]. In terms of family types, mid-range families were the most in this study, followed by balanced and extreme families. This is inconsistent with the previous empirical finding that the balanced families were the most [38, p. 28], and also inconsistent with the assumption proposed by Olson et al. [24] that the mid-range types are dynamically less frequent while the balanced and extreme types are the most common. These differences might be explained by sample differences, and also be related to Chinese culture.
The philosophy of Confucianism emphasizes on individual growth and inspires individuals to strive for getting along with others in harmony posterior to encountering difficulty [29], which may encourage Chinese caregivers to deal with their problems effectively [18] and promotes family bonding and stability because of familism culture. Familism includes feelings of loyalty, reciprocity, and solidarity among members that promotes family cohesion [28]. In a word, the cultural belief might affect some families make sense of the impact of ASD on their family [18; 34]. Altiere and Von Kluge [1] reported enmeshed families (with higher level of family cohesion) generally implemented more positive coping strategies than other cohesion styles. However, due to the neuro- developmental nature of ASD, neither current pharmacological or psychological interventions will completely alleviate children's social and behavioral problems, nor will interventions directed at the children (e.g., social skills training) and the parents (e.g., parent management training) be fully effective [26]. Subsequently, caregivers of individuals with ASD reported more maladaptive behaviour problems and lower personal well-being when compared with those raising individuals with other disability [2]. Besides, Chinese families of children with ASD perceived relatively limited support [22; 33], and they may even be reluctant to seek help from outside supports and resources [18] because of their desire to protect the well-being of the “ingroup” and to “save face” [34], which make it difficult for family members to adapt to pressure. As Lin et al. [18] reported Taiwanese mothers of individuals with ASD showed greater use of emotion-focused coping strategies (i.e., an attempt to regulate the emotional responses to the stressful situations, which was related to negative caregiver perceptions) because they perceived the conditions to be unalterable, which accounted for their lower levels of family adaptability and higher levels of depressive symptoms. Thus, most families in this study tended to show balanced in family cohesion while unbalanced in adaptability. The findings of the study highlight the need of services to be focused on family adaptability and the provision of support to help enhance coping ability.
4.2. Influencing factors of family cohesion and adaptability
Another objective was to depict the factors that affect family cohesion and adaptability. Inconsistent with Rao and Beidel's [26] finding that higher intellectual functioning does not appear to compensate for, nor ameliorate, the behavioral problems associated with ASD, and parents of children with high-functioning autism have restricted family functioning, this study lent evidence that children's functional level had significant effect on their caregivers' family cohesion and adaptability. As Sikora et al. [30] found moderately strong associations between higher externalizing behaviors and poorer family functioning, and the most significant associations among child behavior and increased negativity in parenting perceptions and poorer social functioning. It means family functioning is affected by child's disability characteristics [13; 30]. In addition, caregivers' perceived family cohesion and adaptability did not reach statistical significant differences on children's genders and ages. It might suggest the family functions do not vary significantly depending on child's gender or age. Even though the differences were not significant, it's worthy noting that caregivers with male sons scored higher on family cohesion and adaptability than those with female daughters. It supports the findings of Iacolino et al. [13] that the parents who have male sons showed high scores on family adaptability. But our finding did not support their results that the parents of disable daughters showed significantly higher on cohesion. However, it suggests family functioning when there is a disabled child might be affected by child's gender [13]. Caregivers with older children in the current study scored higher on family cohesion, but lower on adaptability than those with younger children. This is similar to the finding of Iacolino et al. [13] that mothers with older disabled children get higher scores on cohesion. These findings could be used for the support programme for families with children with different characteristics.
Caregivers' marital status also had significant impact on their perceived cohesion and adaptability in this study. Persons who are married or live with a partner scored higher in both the scales. This provides evidence to the research conducted by Zhou [38, p. 35] and Chen [4, p. 29]. And the group of caregivers with higher educational levels had significant higher scores on family cohesion and adaptability when compared to the lower educational levels group, which is consistent with the research results conducted by Zhou [38, p. 31] and Zhang et al. [36]. Caregivers with higher education levels hold higher expectations for their children with disability and could actively acquire as many special education books as possible, so they could choose a more active way to deal with problems associated with ASD [12] and are more likely to get more positive outcomes. Moreover, this study lent evidence to support prior findings that the employment status had impact on family functioning [4, p. 30] and that regular employment helped to reduce caregivers' distress [21] and to enhance parental quality of life [32].
Significant group differences in caregivers' perceived family cohesion and adaptability were found in this study when comparing places of residence, which was similar to the findings of Chen [4, p. 30], Gao [8, p. 23] and Zhou et al.[39]. Families living in cities showed higher levels of family cohesion and adaptability than those living in towns and villages. As Xiong and Sun [33] reported that education resources in big cities were relatively abundant, while those in small towns and rural areas were insufficient. This could be related to different levels of family cohesion and adaptability in different places. In addition, there were significant differences in family cohesion and adaptability while comparing levels of family monthly income. This outcome is consistent with the research results of Chi et al. [5], Zhang et al. [36] and Zhou et al.[39], indicating that family economic status was an important factor affecting level of family cohesion.
4.3. Implications for practice
The findings of this study highlight the need of strengthening family functioning since families were best served by a balanced cohesion and adaptability [23]. Social support has been proved to promote family cohesion and adaptability [7; 37]. As the stress associated with ASD impacts on most aspects of families' lives, such as recreation activities, housekeeping, finances, emotional and mental health of caregivers, marital relationships, physical health of family members, sibling relations and relationships with extended family, friends and neighbors [11]. The chief needs of supports for families of children with developmental disabilities included information, professional service, psychological support, financial demands, and the social services in the community [18]. So this support may include psychological counseling services, educational services, financial support, and even personal assistance and parenting support.
Specifically, the corresponding counseling services should be strengthened to ensure that caregivers' family cohesion and adaptability are at a more favorable level. Mental health service centers can be established to provide systematic, professional, and continuous psychological counseling services for family members of children with ASD [15]. The treatment should focus on improving parent perceptions of their child's diagnosis as well as their feelings about parenting and marital satisfaction [30].
It was reported that the professional education support for children with ASD was the most expected by families [33], so there is a need to provide the information about registered organizations and the methods about how to intervene children. But the systematic planning of services development should focus also on support of other family members and the family as a whole.
In addition, because of low adaptability scores and insufficient monthly income in many families (see section 2.2), it would be beneficent to increase financial and material support for these families, such as providing higher transportation, medical care, and education subsidies. As the time and energy demands placed on caregivers by the child with ASD severely limits their free time and ability to engage in social activities [11], assistance and parenting support can also be provided.
These services may be donated by the government with the aim to train professionals or volunteers providing respite care services for hours, days or even longer, so as to help the family reduce mental stress and return to normal life [16]. The effective development of social support services is expected to help improve the family functioning, and then be beneficial for creating more balanced family environment for children with ASD.
The factors for prediction of the level of family cohesion and adaptability described in this study may be used to improve existing services. These factors may help to assess effectively the problems and needs in the family functioning and to offer adequate strategies for psychosocial support in the counseling practice.
4.4. Limitations and recommendations for future research
This study extends the existing literature by providing considerable and valuable information of family cohesion and adaptability in caregivers having a child with ASD in different social — cultural context. It must be noted, however, that the sampling procedure was limited by several problems, e.g., the willingness of caregivers to participate and provide data or the problem to reach many families of children with ASD. These complications didn't allowed for the creation of a representative and large enough sample to ensure the highest validity of findings. Demographic character of the study (limited on the Sichuan province) makes it difficult to generalize the predictive value of findings outside this region. Thus, it is necessary to prove its predictive efficacy in further studies from other regions. Moreover, this study examined the characteristics of the child, caregiver, and family as the predictors of family cohesion and adaptability. As Iacolino et al. [13] indicated a number of factors appeared to influence the overall functioning of a family with a disabled child, including: the type of disability, the amount and nature of disability-related disorders, the structural and psychological characteristics of the family and the related emotional, relational and educational dynamics, the socio — cultural level and the quantity and quality of social supports that the family has. And Sikora et al. [30] indicated both parent and child characteristics (including chronic health conditions, psychopathology, temperament, level of support, and reaction to stress) and certain family characteristics (such as perceived parenting and social support) all influenced family functioning. Future researches are therefore needed to further evaluate other factors that may influence family functioning such as caregiver mental health and social support and so on.
5. Conclusions
This study examined the perception that Chinese caregivers of children with ASD have of their family functioning and underlined the importance of child, caregiver, and family characteristics on the caregivers' perceived family cohesion and adaptability. The findings of this study justify the need to strengthen the support programme to enhance family functioning in families of children with ASD.