Introduction
With a high reproduction number, mean R0 of 3.28 across China [Liu, 2020], SARS-CoV-2 was a ticking pandemic time bomb from the time it first emerged in December, 2019 in Wuhan, China. WHO declared COVID-19 to be a pandemic on March 11, 2020, and in just about 6 months, on September 18, globally the number of COVID-19 cases surpassed 30 million, according to figures released by Johns Hopkins University.
While lockdown and social distancing emerged as the global strategy to fight the spread of COVID-19, the success of such measures in slowing down or stopping the spread ultimately depends on people's response to such preventive measures. The ability to predict compliance behavior of individuals in response to the COVID-19 crisis could pave the way for designing better communication and intervention strategies to save lives and improve the returns on the economic costs of lockdown.
In planning research on health behavior change strategies, the researcher is faced with a profusion of theoretical frameworks that seek to explain the emergence of self-preventive health behavior. Summarized somewhat differently by different authors [Biddle, 2000; Epton, 2013; Mukherjee, 2013; Ngueutsa, 2017], these include: the Behavioral Decisions Theory [Edwards, 1961], Protection Motivation Theory [Maddux, 1983], Health Belief Model [Bhattacharji, 1982; Rosenstock, 1974], Theory of Reasoned Action [Fishbein, Martin, and, 2011], Theory of Planned Behavior [Ajzen, 1986], an Integrated Model of Behavior Change [Ajzen, 2000], Social Cognitive Theory [Bandura, 1986], Transtheoretical Model [Prochaska, 1983], Extended Parallel Process Model, which attempts to integrate the large array of the Fear Appeal Theories [Witte, 1994], among others. One theory that stands out in this ensemble cast, by virtue of the sheer amount of attention it has received from researchers, is the Health Belief Model.
Since Hochbaum [Hochbaum, 1958] first reported in 1958 that ‘perceived susceptibility' to TB, along with other health beliefs, differentiated between those who went for chest X- ray screening and those who did not [Abraham, 2005], an extensive and impressive body of research was built upon the role of Risk Perception and other components of the Health Belief Model. Over the last 50 years, the Health Belief Model has been “one of the most widely applied conceptual model in the health behavior domain for both explaining and designing interventions related to health behavior change” [Skinner, 2015]. The focus on the Health Belief Model and the role of perceived risk within it continues to this day.
The Health Belief Model (HBM) was developed in the 1950s, in response to the challenge faced by the US public health service in getting people to opt for early detection tests or other preventive steps for asymptomatic diseases [Rosenstock, 1974]. In its original form HBM postulated a set of five factors that were needed to propel people to action. 1) Perceived susceptibility to a disease, 2) Perceived severity of the disease, 3) Perceived benefit in taking the recommended preventive action; 4) Low perceived barrier (e.g., cost, inconvenience, pain, embarrassment, etc.) to taking the recommended preventive action; 5) A trigger (e.g., campaigns by health authorities) to instigate the preventive action.
The model evolved and expanded over time to include other risk perception elements. The original construct of perceived susceptibility comprised a cognitive estimate by the respondents of their likelihood of contracting a disease. Slovic et al., [Slovic, 2004] pointed out that risk is perceived in two main ways: A) as a cognitive “analysis” of the probability judgment of danger and B) as an affective element he called ‘affect heuristic'; and that decision making involves the integration of “both modes of thought”. Within the affective element of risk perception, Loewenstein et al. [Loewenstein, 2001] made a distinction between “anticipatory” emotions (e.g., fear or anxiety) about the possibility of harm, and “anticipated” emotions (e.g. regret or guilt) about the “expected consequences of the decision”. Brewer et al., [Brewer, 2007] reported that in addition to anxiety and regret, vaccination behavior increased with the increasing ‘feeling at risk' and as such it could be a better predictor of self-protective behaviors such as vaccination than cognitive judgment of probability of risk. The initial conceptualization and operationalization of the risk perception construct, which was limited to only its analytical, cognitive element to the exclusion of the affective/experiential elements is one of the reasons that many meta-analytic studies, [e.g., 10; 29; 31] found a significant but only modest association between perceived risk, intentions and behavior [Epton, 2013]. In the same meta-analytic review of experimental studies on risk perception, Epton et al., [Epton, 2013] also reported that “messages that successfully heightened more than one of these elements of risk appraisal had larger effects on outcomes than messages that heightened only a single element”.
The current theoretical development emphasizes a further distinction between the affective and the experiential elements of risk perception, as these two elements access and employ different information processing systems. The experiential component of risk perception has been described in the TriRisk model by Ferrer et al., [Ferrer, 2016] as:
“rapid, heuristic-based judgments that involve “ ‘gut-level reactions' ” and “as neither rule-based, logical assessments nor fully-fledged affective responses; they are outputs of experiential processing that is holistic, based on learned associations, slow to change, relatively crudely differentiated and integrated, and involving concrete images, metaphors, and narratives”.
These descriptions are based on previous conceptualization by other authors [15; 20;
63; 73]. Ferrer and her colleagues [Ferrer, 2016] do not provide a differential definition of their own. While the description might seem to lack clarity [Wilson, 2019], the operationalization of the experiential risk perception the TriRisk model is quite clear. It has been operationalized and measured as a ‘gut-level perception of vulnerability to a given health risk' [Ferrer, 2018]. They reported A) better model fit with the TriRisk model compared to single-factor or two-factor models; B) improved predictive validity, and C) important implications for targeting risk perception in health behavior change interventions.
How Do the Three Risk Processes Work?
In addition to asking ‘when', the second-generation research question [Zanna, 1982] also asks ‘How'? How does the process work? “What mediates the effect?” The ‘How' question is indeed an important one as it is likely to throw further light on how the three different risk perceptions work together to influence self-protective compliance behavior. More importantly, from the translational perspective, any evidence of such mediational effect is likely to have implications in framing communication messages for disease transmission reduction interventions.
Literature is rather sparse in this area. Some evidence was provided by Chapman & Coups [Chapman, 2006], who reported that anticipated emotions, regret and worry, mediated the relationship between cognitive risk estimation and vaccination. Slovic et al. [Slovic, 2004] summarised some of the major empirical evidence to argue that the analytical processing of risk cannot be effective unless aided and guided by affect and emotion. They suggest a continuous interplay of the experiential, affective and deliberative processes in what they called “the dance of affect and reason” [Finucane, 2003], though they subsumed the affective and the experiential components in a single category, under the “two-mode thinking” conceptualization.
Support for the interplay between the deliberative processes and the experiential- affective processes comes from the neuroscience domain in the form of comparing hemodynamic activity in the brain. Mohr et al. [Mohr, 2010] based on their meta-analyses of 30 functional magnetic resonance imaging (fMRI) experiments, suggested that both the affective and the analytical risk-processing mechanisms work together in consort with one another.
Exposure to a risky situation triggers both the cognitive and affective risk assessment processes. Throughout the sequence, the aINS and thalamus (executing the experiential- affective risk estimation) and the dmPFC (executing the cognitive- analytical path) keep talking to each other until the dorsolateral prefrontal cortex (dlPFC) integrates the risk information with other pertinent information to make an action decision. The results of the me- ta-analysis, authors note, are consistent with the essential postulates of the risk- as-feelings hypothesis [Loewenstein, 2001]. Yet other investigations in the neurophysiological domain point to the direction of a stronger affect-to-cognitive path than the reverse path from cognitive to affect [LeDoux, 1996]. But the most direct and unambiguous observation comes from Loewenstein who noted: “Diverse evidence also supports the proposition that affect mediates, at least in part, the relationship between an individual's cognitive evaluation of risk and his or her behavioral response to it” [Loewenstein, 2001]. One of the clearest reviews of conceptualization and research in this area, Kiviniemi et al., [Kiviniemi, 2018] points out the limiting nature of the large body of mainstream research that treats affect and cognition as two isolated groups and attempts to investigate their effects on health behaviors as separately transmitted main effects, ignoring the complex interplay between them.

Fatalism
“My first encounter with fatalism in practice took place thirty years back when a maidservant who was absent for a week said on her return that her two-year-old son had died of smallpox. When I asked her whether he had been vaccinated against it she said in a piously resigned tone that since the boy was ‘fated' to die of smallpox no vaccination would have prevented his death. Of course, this attitude is born of ignorance, but what shocked me was her acceptance of the death and the peace and consolation she derived from this acceptance” [7, p. 135].
Another theoretical framework that has been the subject of considerable research in relation to health behaviors is Fatalism. Bhattacharji [Bhattacharji, 1982] in her comprehensive treatise, described fatalism essentially as an “emphasis on the incalculable above the predictable” and analysed its interconnected facets that included, among others, predetermination, acceptance of one's situation, a coping mechanism, and “revolt against intellectualism, especially where rationality or intellectualism fails to solve certain problems”. Other authors have defined fatalism variously, depending on their conceptualization and operationalization perspective, that inter alia includes elements of predetermination [Ross, 1983], external locus of control [Wheaton, 1983], acceptance of one's situation [Futa, 2006], lack of personal control over destiny [Drew, 2011], and inevitability of unfortunate events [Ngueutsa, 2017].
The divergence in the operationalisation of fatalism has been reflected in the approach to its measurement. Esparza [Esparza, 2005] reported the existence of 51 different purported scales of fatalism with little convergence in their operational definitions. To integrate the different dimensions of fatalism, Esparza et al., [Esparza, 2015] developed a multidimensional fatalism scale that captured the different dimensions of fatalism under 5 subscales: fatalism, helplessness, internal- ity, luck, and divine control. According to the authors, the first subscale — fatalism — embodies the core of the fatalism construct and should be the primary target of fatalism research. This subscale measures the “tendency to view all events as fixed in advance and inevitable”, which closely approximates the idea of fatalism as it has existed in the traditional Indian belief system. Bhattacha- rji [Bhattacharji, 1982] expressed the idea eloquently with the oft-repeated Sanskrit saying: “Niyatih Kena baddhyate”, which means “fate is incontrovertible — ... acquiescence to Fate Supreme.”
Fatalism has been studied from diverse perspectives including, anthropological, sociological, and psychological perspectives. Within the health behavior research domain, the role of fatalism vis-a-vis health behaviors have been considered mainly from two explanatory standpoints. The first involves control beliefs and is related to the constructs of locus of control [Rotter, 1966], and self-efficacy belief [Bandura, 1986]. Authors such as Straughan, [Straughan, 1998], proposed that fatalism influences self-efficacy, which in turn affects health behavior. They also argued that the social cognitive theory [Bandura, 1986] provided a more useful model for studying health behavior than rational choice models. The second standpoint, advanced by authors like Powe [Noar, 2005; Powe, 1997], Lange & Piette [Lange, 2006], has treated fatalism as a potential barrier to health behavior that needs to be modified for health behavior change interventions. Looked at from either standpoint, fatalism appears to be a useful construct to investigate together with HBM in attempts to predict self- protective health behavior. It is becoming increasingly more common for researchers to integrate constructs from different theoretical models in investigations involving HBM [Skinner, 2015].
The present study
While both the HBM, and to a somewhat lesser degree, the construct of fatalism have been tested and applied in a wide range of diseases and health issues, the CO- VID-19 disease presents a very different set of dynamics, unlike anything hitherto known or seen. A disease, where the recommended health behaviors limit lives and livelihoods of people en masse by requiring extensive social isolation with its inevitable economic and emotional fallouts. This vastly different dynamics of the COVID-19 disease make it imperative to examine afresh the applicability of a model like HBM that has been applied in a wide variety of other health issues. Thus, the present study:
1. Has a predominantly translational focus: to examine the applicability/transfer- ability of the constructs of the HBM, the TriRisk model [Ferrer, 2016], and fatalism-belief in the context of the COVID-19 disease, specifically to test if they help us predict preventive compliance behavior.
2. We also bring together the constructs of the HBM, TriRisk model, and fatalism under the same investigative umbrella for the first time, to the best of our knowledge.
Furthermore, we examine through mediation analysis how the three components of the TriRisk model work together, again for the first time, to the best of our knowledge.
3. With the translational goal in mind, we have consciously desisted from constructing elaborately formal hypotheses and making narrowly formulated a priori predictions, replacing them with testing expectations in relatively broader general directions, which are listed below:
We expect the basic components of HBM, the TriRisk model and fatalism to apply in the context of the COVID-19 disease. Specifically, and additionally:
1. All three risk components, viz., deliberative, affective, and experiential to be positively associated with and predict compliance behavior.
2. Benefits to be positively associated and barriers negatively, with compliance behavior.
3. Fatalism to be negatively associated with compliance behavior.
4. Finally, we intend to examine the interplay among the three risk perception components in the light of existing theoretical directions and available evidence.
Methods and materials
Participants
357 Participants from different parts of India responded to an invitation circulated through different online platforms that included social networking media and communication channels, such as LinkedIn, Facebook, Twitter, WhatsApp, email, etc., to participate in an online survey using the online google platform. The age range of participants were 15—78 years (M=47.64, SD=14.46), 41.5% of whom were men and 58.5% were women. Approximately 39% of the participants were from containment zones (hotspots) and 61% were from noncontainment zones. The data were collected during May and June 2020, the complete lockdown phase in India. The demographic details of the participants [N=357] are available on request.
Measures
Both multi-item and single-item scales were used in the present study. Though multi-item scales are generally preferred, we wanted to reduce the burden on respondents as much as possible, as the study was conducted during the complete nationwide lockdowns when peoples' lives were in a state of complete economic and psychological topsy-turvy. Hence, we decided to use single-item scales wherever possible. Use of single-item scales has been found to be justified on grounds of practicality, reduced burden, cost, and ease of interpretation [Bowling, 2005]. Weinstein et al., [Weinstein, 2007] specifically investigated the ability of several types of risk perception measures and of other constructs from health behavior theories to predict self-protective compliance behavior. They also compared single-item and multi-item scales to investigate their relative performance. Their conclusion was: “In this domain, a well-chosen single item scale can predict just as well as multi-item scale” [70, p. 150]. Single- item scales in this area have been used by other researchers e.g., Ferrer et al. [Ferrer, 2015], as well. The scales used are described below. A full list of the items is available on the Appendix.
1. Deliberative risk perception: Diefen- bach et al. [Diefenbach, 1993] and Weinstein et al. [Weinstein, 2007] reported that the 7-point scale performed best in assessing risk magnitude when compared to dichotomous item, percentage item and 6-point forced-choice item scales Based on this evidence, a single item 7-point scale was used that required participants to estimate the degree of risk probability by choosing from options that ranged from “almost zero” (=1) to “almost certain” (=7).
2. Experiential risk perception: Experiential risk perception measured the ‘gut-level feeling of being at risk', assessed by a singleitem 5-point scale.
Affective risk perception: Affective risk perception measured the elements of anxiety, fear (of putting family members at risk), and anticipated regret with a multi-item 5-point scale. Item scores were added to generate a composite affective risk perception score. Cronbach's alpha is not an appropriate statistic in this case, as it is highly sensitive to the length of a scale. Mean inter-item correlation can give a better estimate of internal consistency and an optimal range from .20 to .40 has been suggested [Briggs, 1986]. The mean interitem correlation of the affective risk perception scale is .27.
3. Perceived severity: captured the perceived seriousness of the consequences (hospitalization, being put on ventilation, etc.) of contracting COVID-19. A single item scale with 5 response categories was used to assess perceived severity.
4. Perceived Barriers: This scale assessed the perceived obstacles (difficulty) in complying with the recommended preventive measures on a single-item 5-point scale.
5. Perceived Benefit: Participants responded to a single question on the effectiveness of the recommended lockdown and social distancing guidelines in preventing the COVID infection by choosing from options that ranged from “not at all effective” (=1) to “very effective” (=5).
6. Fatalism: The six-item ‘Fatalism' scale, a subscale of the Multidimensional Fatalism Measure developed by O.A. Esparza et al. [Esparza, 2015], was used to measure the fatalism dimension. The authors describe this scale as measuring the “tendency to view all events as fixed in advance and inevitable”. The scale has 6 items requiring a response on a 5-point “strongly disagree” (=1) to “strongly agree” (=5) scale. The Cronbach alpha for the present study sample was found to be .89.
7. Compliance behavior: is the dependent variable in the present study. It comprised 7 items that measured the extent to which respondents had been complying with the various guidelines on lockdown- related preventive measures issued by the government, such as staying at home, social distancing, wearing masks in public, maintaining personal hygiene, etc. Response options for each item ranged from “Not at all” (=0) to “completely” (=10). The composite compliance behavior score was derived by adding all the item scores. The Cronbach's alpha for the sample was .83. Factor analysis, using principal axis factoring yielded a single factor solution that explained 44.24% of the variance.
8. Demographic variables: captured gender, age, education, income, and COVID hotspot status.
Results and discussion
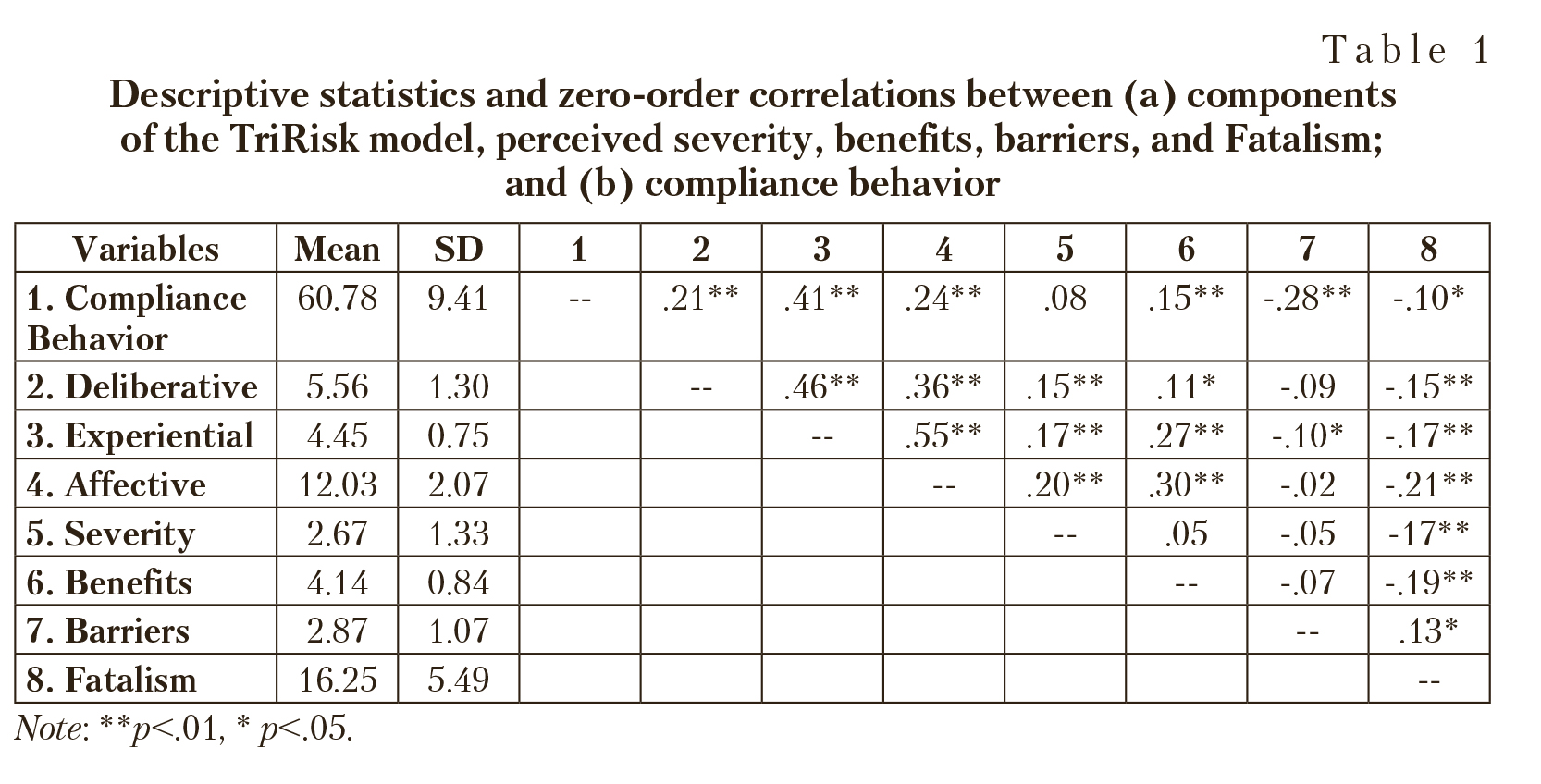
The descriptive statistics and correlations between (a) components of the TriRisk model, perceived severity, benefits, barriers, and Fatalism; and (b) compliance behavior, are presented in Table 1.
The correlations show that the risk perceptions, HBM components, and fatalism are associated with preventive health behavior, as expected. All the three dimensions of TRIRISK model are positively and significantly associated with compliance behavior with experiential risk perception having the strongest association, followed by affective, and deliberative. Perceived benefits are also significantly and positively correlated to compliance behavior while perceived barriers are significantly and negatively associated with compliance behavior, as expected. Very small relationship was observed between perceived severity and compliance behavior — an observation that has been consistently reported in the literature [Carpenter, 2010; Harrison, 1992]. Fatalism was found to be significantly and negatively associated with compliance behavior, as expected. Overall, the patterns of associations between these predictors and health behavior appear to hold good for the COVID-19 pandemic.
Predicting Compliance from TriRisk Model, HBM and Fatalism
The results (significant predictors) are presented in the following tables:
Only three variables, experiential risk perception, perceived barriers, and gender significantly predicted compliance behavior (Table 2). Together, they accounted for some 24% of the total variance. Experiential risk perception was the strongest predictor, followed by barriers, and gender. When the variables were entered in hierarchical models, experiential risk accounted for 17% of the variance. Incorporation of barriers in the equation explained another

additional 5%, and finally, introduction of gender in the model explained a further 2% of the variance.
The fact that deliberative risk perception did not turn out to be a significant predictor of compliance behavior is consistent with Carpenter's [Carpenter, 2010] findings, who in his meta-anal- ysis reported that “susceptibility was a weak predictor of behavior”. That experiential risk perception would predict preventive health behavior was expected and is consistent with evidence available from several studies [Ferrer, 2015; Ferrer, 2018; Ferrer, 2016; Wheaton, 1983]. However, the elements of affective risk perception, viz., anxiety, fear and anticipated regret that have been previously found to be predictors of self- protective behavior and or intentions [Chapman, 2006; Ferrer, 2018; Ferrer, 2016; Weinstein, 2007] did not turn out to be so in the present study. Any discussion about the reason for this divergent finding would be speculative until we know more about the psychological dynamics of the COVID-19 disease.
Though benefits had a statistically significant association (p<.01) with compliance behavior, the effect size was rather small — a finding that is somewhat unexpected as the literature indicates a stronger association [Carpenter, 2010]. Also, we did not find benefits to be a significant predictor of compliance behavior. Again, at the cost of being speculative, it appears that the link between perceived benefits and compliance behavior
could be somewhat tenuous during those early phases when the prevention guidelines were received possibly with incredulity, yet uncritically (the scepticism and the denial would come later); and compliance was to an extent externally enforced.
Barriers have consistently been found to be one of the strongest predictors of both behavior and intention [Carpenter, 2010; Janz, 1984; Rosenstock, 1974]. Though barriers in the context of COVID-19 presented health behavior challenges of a rather unique kind — social isolation — it was found to be a significant predictor of compliance behavior in the present study, as expected. Gender was also found to be a successfull predictor of compliance behavior, wherein women were associated with a significant increase in compliance behavior, compared to men.
Besides experiential risk perception, barriers, and gender, the only other variable that accounted for some additional variance was income. Better health compliance has been shown to be associated with higher income levels in many studies [Habib, 2018; Mukherjee, 2013]. Our results, however, indicate that the relationship may not be as straightforward as it might otherwise seem. Only two income categories (? 60,000 to ? 100,000; and > ? 150,000 per month) significantly predicted an increase in the compliance behavior, while the middle category (? 100,000 to ? 150,000) was not a statistically significant predictor.
Fatalism as a construct has been gaining currency and popularity in the last fifty years or so, and has been the subject of a large body of research involving health behavior. Fatalism has been implicated in failure to adopt self-protective behaviors in a wide variety of health-related areas [De Los Monteros, 2011; Shen, 2009]. Cohn & Esparza [Cohn, 2015] reported that 65% percent of the 46 studies, included in their meta-analysis found “at least one significant relationship in the predicted direction between fatalism and health behavior”. Kishore et al., [Kishore, 2008] reported that in a sample of Indian cancer patients that comprised semi- skilled and skilled workers with no formal education, the majority held some form of fatalistic belief about cancer and its treatment; and that the average time to seek treatment after the disease had been first suspected, was 2 years. Several researchers, [e.g., 40; 53; 54; 69], have suggested that to successfully modify health behaviors, fatalism related beliefs need to be considered.
However, in the present study, though there was a statistically significant negative relationship between fatalism and compliance behavior, fatalism was a weak and non-significant predictor of compliance. In a recent meta-analytic study of fatalism and health behavior, Cohn and Esparza [Cohn, 2015] reported that the average effect size was small (d=0.26) equivalent to a point-biserial correlation of approximately 0.13. They concluded that the relationship between fatalism and health behavior is possibly much smaller than previously thought or expected.
Mediation Analysis
Kiviniemi et al., [Kiviniemi, 2018] recommended that in the interest of building more realistic models, researchers routinely investigate mediating and moderating effects even if such investigations are done post hoc and were not a part of a priori expectations. In addition to multiple linear regression analyses and hierarchical regression models, we conducted exploratory mediation analyses to examine if our data revealed a similar mediational pattern as could be expected from the literature.
To test the mediational interplay of the risk processes, we built three separate parallel mediation models (N=357), using ordinary least square path analysis. In each of the three models, all the predictor variables other than the ones in that model were controlled by entering them as covariates. X by M interactions were included in the equations to test the no-interaction assumption. In line with the current theory and practice [Hayes, 2017; Hayes, 2017a; Rucker, 2011], the estimation of indirect effects and bootstrap confidence intervals, based on 5,000 bootstrap samples, were used to test the mediation effects. All analyses were conducted using SPSS macro, PROCESS, version 3.5. To ensure heteroskedasticity-robust inference testing, we applied HC4 [Cribari-Neto] heteroskedasticity-consistent standard error estimator for OLS regressions in our regression analyses.
In the first model (Figure 2), the total effect of deliberative component on Compliance behavior was positive and significant (c=1.17, p=.009). However, the direct effect was not statistically significant (c'=0.16, p=.676). The first indirect effect between deliberative risk perception and Compliance behavior, mediated through experiential risk perception M1 (a1b1=0.94) while controlling for affective risk perception M2, was entirely above zero, 95% CI (0.357 to 1.628). However, the second mediating variable M2 mediated an indirect effect between deliberative risk perception and Compliance behavior that was (a2b2=0.07) non-significant, 95% CI (-0.195 to 0.372). Results of X by M interaction tests: M1*X, FHC4 (1, 339)=0.01, p=.919 and M2*X, FHC4(1, 339)=0.12, p=.730, support the assumption of no interaction between X and either mediator in this parallel mediator model.

In the second model (Figure 3), almost the entire total effect of experiential risk perception on Compliance behavior (c=4.33, p=.000), was direct effect (c'=4.02, p=.002). There was no evidence of indirect mediation through deliberative risk perception M1 (a1b1=0.13, bootstrap 95% CI: -0.417, 0.765) or through affective risk perception M2 (a2b2=0.18, bootstrap 95% CI: -0.506, 1.015). Results of X by M interaction tests: M1*X, remaining the same as reported in the previous model, and M2*X, FHC4 (1, 339)=0.11, p=.741, support the assumption of no interaction between X and either mediator in this parallel mediator model.
Finally, in the third model (Figure 4), we regressed Compliance behavior on the remaining non-analytical risk perception variable, viz., affective risk perception, and entered deliberative and experiential risk perceptions as proposed mediating variables, M1 and M2, respectively. While the total effect of affective risk perception on compliance behavior was positive and statistically significant (c=0.90, p=.001), it was not through direct effect, which was non-significant (с'=0.14, p=.643). Again, there was no evidence of deliberative risk perception, M1, mediating the relationship between affective risk perception and compliance behavior (a1b1=0.04, bootstrap 95% CI: -0.120, 0.230). That experiential risk perception, M2, mediated the association between affective risk perception and compliance behavior was established through the indirect effect (a2b2=0.72, 95% bootstrap CI: 0.285, 1.126).
The finding that experiential risk evaluation mediated the association between deliberative risk evaluation and Compliance behavior is consistent with the causal flow suggested by Loewenstein [Loewenstein, 2001].
However, the finding that the affective component in the present study that measured both experienced (anxiety, fear) and anticipated (regret) elements of the non-cognitive risk evaluation path did not similarly mediate cognitive risk evaluation, which was putatively expected, merits further investigation in future research.
Limitations
The primary limitation of this study involves the representational aspect of the sample. The data were collected from a convenience sample drawn, using Internetbased channels. In the absence of probability sampling generalisability remains an issue. However, generalisability, as a blanket requirement has been brought into question by several authors who essentially have as

serted that representativeness of samples used need not be a necessary requirement if testing predictions rather than making them is the objective [Mohr, 2010], and that population inference is often not the objective of a study [Hayes, 2017]. The same logic applies to the present study.
Another limitation related to the previous one is that the sample included only those respondents who have access to the Internet and can read English. Though English is one of the two national level official language in India and the second most widely spoken second language in India after Hindi [Registrar general, 2011], its use is linked with education and income levels [Annamalai, 2004]. Thus, those from the lower socioeconomic strata, and those who cannot read English, did not get included in the sample. Using verbal response scales in Hindi or other regional languages in future research would help overcome this limitation, which was not possible during a nation-wide lockdown when the data for the present study were collected.
Concluding Remarks
The essential findings of the present study are:
1. There were only three variables, amongst those we studied, that statistically significantly predicted COVID-related compliance behavior. experiential risk perception, perceived barriers, and gender.
2. Out of these, experiential risk perception was the strongest; it accounted for 17% of the variance in compliance behavior, followed by perceived barrier which explained another 5% variance. Gender accounted for about 2% of the total variance.
3. Though deliberative risk perception, ‘susceptibility' in HBM, and affective risk perception both significantly and positively correlated with compliance behavior, neither of these two turned out to be statistically significant predictors of compliance behavior.
4. Evidence suggested that experiential risk perception mediated the path between cognitive risk assessment and compliance behavior, not vice versa.
If the present study roughly corresponds to a stage somewhere between T0 and T1 in the translational research framework, point numbers 1 through 3 above, have implications for designing and trying out compliance enhancement interventions in the next stage. Use of appropriate experiential risk content in designing public campaigns and advisories is a strategy that merits further attention. No doubt, the hardest of barriers is economic in nature and structural support from governments by way of economic packages and other similar measures are needed to tide over the life versus livelihood conundrum. However, Reduction of perceived barriers through reassurances, dispelling misinformation, and providing assistance [Skinner, 2015] will potentially supplement the structural support.
Our findings — that experiential risk perception mediated the cognitive risk path to compliance — (point number 4), helps in understanding the nature of interplay between gut level sensing of risk and analytical risk assessment, vis-a-vis self- protective behavior. Loewenstein et al., [Loewenstein, 2001] noted that “...these rapid emotional reactions serve as a mechanism to interrupt and redirect cognitive processing toward potentially high-priority concerns, such as imminent sources of danger.” Considering the fact that threat from infectious diseases has had a long history and has played a role in human evolution for more than 5 million years [Rucker, 2011], it stands to reason that a deadly pandemic like COVID could activate what LeDoux [LeDoux, 2012; LeDoux, 2014] called the “survival circuit”. A process that kicks in, when significant challenges or opportunities in the environment are detected, and initiate actions to help self-preservation.
In conclusion, we are aware that crosssectional design and correlational analyses do not provide sufficient basis for making causal inferences. And that was not the objective of the present study. We attempted to discern patterns in the available data — patterns that could provide some clue in designing campaigns to promote social distancing and related preventive measures. Establishing cause-effect relationships is the holy grail of science. Doing that even through a series of experimental manipulations may not always be fool proof as establishing equivalence convincingly between two experiments in a series may not be possible [Slovic, 2005]. The present study
was conducted during the first complete lockdown in India when the entire country was shut down 24x7 for more than two months, which put severe constraints on data collection and alternate designs. But as Hayes [Hayes, 2017a] commented, “we should not let the limitations of our data collection efforts constrain the tools we bring to the task of trying to understand what our data might be telling us about the processes we are studying.” The practical implication of our findings points towards an increased importance that experiential risk perception merits in designing campaigns to promote social distancing and related preventive measures.