Evidential Reliability Post-CPR
Since the implementation of the UK-based Civil Procedure Rules in 1999, fifteen years have passed with the courts, lawyers and experts getting to grips with the various changes and their implications, and the aims to ensure access to justice which was just, fair, appropriate and effective.
1. In general, the implementation of CPR has led to improved access to expert evidence [fairness, cheaper, quicker, easier to understand].
2. Experts have been more focused on restricting evidence to ‘what is reasonably required to help resolve proceedings.
3. Experts restrict their evidence to evidence which is ‘within their expertise’.
4. Process of getting answers to written questions from experts is timely, helpful/accurate.
5. The content of reports reflects an increased independence of experts and increased responsibility to the Court.
6. Reports reflect the appropriate range of opinion.
The Medico-legal trail and key questions
a. The medico-legal trail
Below is a flow chart which illustrates the key aspects of the medico-legal decision making process from instruction of a claim to its resolution (Koch et al, 2015).
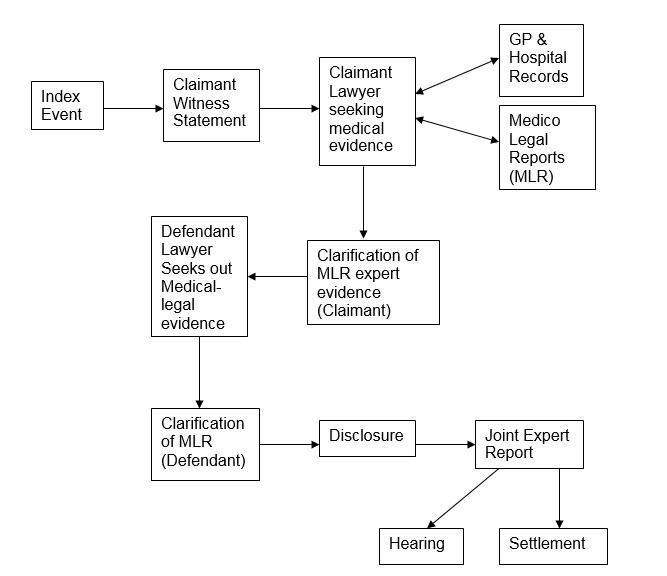
Fig. 1. The Medico-Legal trail
b. The key medico-legal questions
A medico legal expert frequently interviews a claimant to establish the injury, psychological or physical, that has occurred, and whether this is attributable to the index event. Seven key medico-legal questions are shown in Figure 2 (Koch at Kevan, 2005). Interview information, witness statements and medical and occupational medical records, provide the expert with an array of ‘data’ which he/she diligently considers in order to arrive at the most logical opinion.
|
1) What, if any, injuries or medical conditions resulted from the claimants’ accident? |
|
2) Are these injuries and conditions consistent with / attributable to this accident? |
|
3) Are there any symptoms that relate to pre-existing conditions, and to what extent have these been exacerbated by the accident or made the claimant vulnerable to the accident related injuries? |
|
4) What was the course and duration of these injuries and medical conditions to date, and were these within the expected range? |
|
5) Was any absence from work in light of the injuries sustained reasonable? |
|
6) What treatment has already been received and/or is likely to be needed in the future for these conditions? |
|
7) What is the likely extent and duration of any continuing disability? |
Fig. 2. The Key Medico-legal questions
The opinion is then ‘tested’ via claimant response, lawyer clarification and debate, followed by between-expert discussion, before occasionally being tested in Court. Throughout this process there are two factors which the expert must grapple with to arrive at a ‘best-fit’ opinion – reliability and validity.
Improving Evidential Reliability
When assessing evidential reliability, the Law Commission (in 2011) stated that experts should have regard to a number of factors including:
A) The extent and quality of the data on which the opinion is based;
B) If the opinion relies on an inference from any findings, and whether the opinion explains how safe or unsafe the inference is;
C) If the opinion relies on the results of the use of any method (for instance, a test or survey), whether the opinion takes proper account of matters, such as the degree of precision or margin or uncertainty, affecting the accuracy or reliability of those results;
D) The extent to which any material upon which the opinion is based has been reviewed by others with relevant expertise and the views of those others on the material;
E) The extent to which the opinion is based on material falling outside the expert’s own field of expertise e.g. organicity of pain.
F) The completeness of the information which was available to the expert, and whether the expert took account of all relevant information in arriving at the opinion.
G) Whether there is a range of expert opinion on the matter in question; and if there is, where in the range of opinion lies and whether the expert’s preference for the opinion proffered has been properly explained.
The use of diagnostic classifications (e.g. DSM V) of disorders have significantly improved the reliability and validity of diagnosis, where symptoms can be aligned to a ‘best fit’ diagnosis which can be communicated and discussed between expert and with the Court. However, the Courts should be encouraged to compensate individuals according to disability (i.e. actual loss) and disruption rather than purely a technical diagnosis.
Within the interview, the clinician listens for descriptions of symptoms which appear unsound or unreliable. The most common indicators of unreliability are shown in Table 1 below.
Table 1
Indicators of unreliability
|
(a) “Blanket” problems and gross symptoms claiming |
|
Almost all areas of enquiry produced claiming discomfort. |
|
(b) Selective Recall |
|
Poor recall of pre-accident traumas (e.g. previous accidents or minimising of pre-accident stress). |
|
Difficulty acknowledging evidence of recent improvement in distress or functioning. |
|
(c) Magnifying Recall |
|
Use of a single example only to reflect apparent consistent and sustained distress (e.g. when I drove the first time after the accident it was awful). |
|
(d) Discrepancy between self-report and other evidence |
|
between client and GP information. |
|
between client and work information. |
|
between client and relative information |
|
(e) Production of rare or common symptoms |
|
Claiming unusual, strange, atypical or preposterous symptoms. |
|
Claiming symptoms which are experience by most of the general population (e.g. losing objects, forgetting names occasionally). |
a. Thorough clinical interviewing and data gathering
The expert clinician, like the expert lawyer, develops skills over time in “listening” to available information and organising a “picture” of an individual containing:-
(a) facts about the trauma and its after effects;
(b) the individual’s perception of his/distress (physical and psychological);
(c) significant other’s perception of the individual (e.g. family, other experts, GP);
(d) an appraisal of reliable behavioural data on ability and disability; “I can’t lift things” or “I can’t drive” must be backed up by examples of previous behaviours which are now avoided (partially/totally) and frequency of such avoidance to reflect level of disruption.
(e) ‘Networking’ with other experts and/or available reports to try and not only present one expert view, but also facilitate a development of the overall picture of an individual across clinical disciplines/functions (e.g. orthopaedic, neurological or psychological).
b. Comparison of claimant history and symptoms with GP records
The expert is typically presented with several different sources of medical and occupational records. However, frequently the most useful is the GP medical journal of attendance (typically computerised for more recent years). This gives the expert the opportunity to compare what the claimant has disclosed either through interview or witness statement about: a) their condition and b) their GP attendance (Koch and Mackinnon 2004).
One key question remains: whether the Claimant would have attended their GP for diagnosis and treatment if they had a clinically significant psychological injury? Some clue to this can be found in their previous records; if they previously attended for psychological problems, there is unlikely to be a post index incident reason why they have not attended unless their condition is very mild or absent.
A formal GP chronology (typed and complete as far as possible) is essential to enable the experts on both sides to, sensibly and logically, answer pertinent questions in a non-partisan, objective manner. What does the pattern of attending indicate about:
-
Pre-accident status
-
Immediate post accident experience
-
Diagnostic and treatment provided
-
Other factors cited (related or unrelated)
-
Duration of symptoms and treatment?
c. How can reliability and validity be enhanced?
Ultimately, any ‘certainty’ of evidence depends on whether it is consistent with the probabilities affecting the case as a whole and shown to be in existence at the time.
Findings of credibility and reliability require a comprehensive and critical examination of the evidence as a whole – not only one element to the exclusion of others.
When investigating characteristics of reliability and validity in claimant’s interviewing content and style, there are several aspects of the patient history which are addressed:
-
Pre accident condition and psychosocial context.
-
Index trauma and peri-traumatic context (soon after).
-
Immediate short term reaction and level of disruption.
-
Natural improvement.
-
Prognosis and change/treatment expectations.
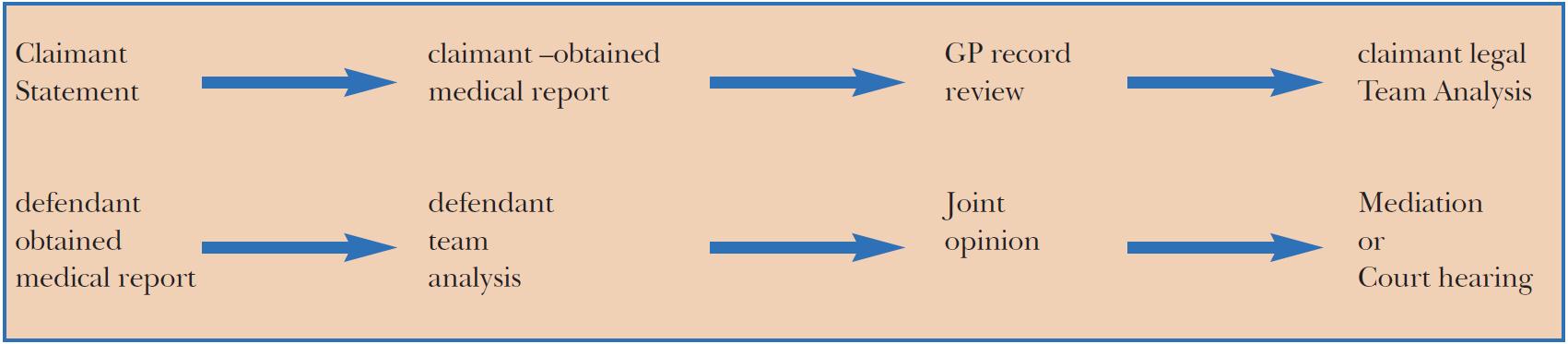
Fig. 3. The current litigation process increases ‘evidential certainty’ as it progresses. The typical ‘trail’
During this process, there is a search for the ‘best fit’ opinion. With regards to increasing objective and contemporaneous information, if all Claimants are expected to have attended their GP or equivalent at the earliest possible time post-index accident, this would provide a contemporaneous and independent record from the GP of physical or psychological injuries and causation. It seems suspicious when the trail of complaint only begins with the commencement of litigation.
It should be remembered that it is incumbent on the claimant (or his/her representatives) to “prove” the case of attributing injury to the index event. However, the role of single event trauma can be over emphasised and co-existing psychosocial factors which are unrelated to the trauma may be both critical and under estimated.
It is important to place and compare the claimant’s overall ‘picture’ into the context of epidemiology, normality, common sense and what is called a ‘default mode’ – in plain English, what sort of reaction would be expected to be found in the general population. This must be particularly the case when dealing with adjustment reactions/disorders, or where a whole family complains of the same psychopathology.
In this context it is important to remember and apply the ‘But For’ test to decide objectively the relevance of pre-index event history. However, claimants may have difficulty recalling their history comprehensively, thus making the expert’s ability to apply the ‘But For’ rule difficult and consequently, less reliable.
d. Evidential Reliability in Psychological/Psychiatric Opinion
Experts in psychology/psychiatry are aware that there are several sources of unreliability at play when conducting medico-legal interviews, preparing their opinion and also when conducting joint opinion discussions.
In order to clarify what some of these sources are specifically, we conducted a survey of 40 experts in the field of psychology and psychiatry to ascertain which factors predicted, in their opinion, unreliability.
This data indicated that several aspects of claimant recall account for a significant level of evidential unreliability with recent memory difficulties plus magnification/exaggeration being two principal factors.
Experts themselves contribute to evidential unreliability in terms of non- specificity of symptom assessment (symptoms overlapping), over-selectivity of areas covered, over reliance of self report data and differences in data defining symptom duration, pre-existing history and review of GP records.
These several sources of unreliability are a major factor contributing to levels of disagreement between experts when they come to discuss an prepare joint opinion schedules.
Experts were also asked about ways to improve or enhance the reliability of psychological/psychiatric options. These included: Clearer definition of diagnostic criteria, Increased structure of Interview, Use of symptom rating scales in interview and Training and CPD Opportunities
Work is currently underway to clarify the key differentiating factors between the main or typical psychological disorders and how to assess the level of disruption these cause. A key finding in the above study was the need or benefit from further training and CPD opportunities for experts in the field of psychology and psychiatry. In all probability, these benefits would also apply to other clinical specialties (Koch et al 2015).
Unreliable pre-index accident history
Interviewing claimants in Personal Injury litigation frequently entails being faced with ambiguous pre-accident history, due predominantly to unreliable or inaccurate recall (Koch and Kevan, 2005).
The expert is faced with two dilemmas: what is true and accurate, and secondly, does this ambiguity reflect credibility and/or truthfulness issues.
Case Studies
The following case studies are examples from the two authors’ own medico-legal practices and illustrate how ambiguity and unreliability arises:
|
Vignette 1: |
|
The claimant, when asked, stated he had never had any previous car accident before the index accident. He also stated he had never brought a claim for personal injuries before. When given the data in his GP notes about a traffic accident 7 years before, he ‘remembered’ this. He did not dispute the evidence but was vague with details. He was apologetic and gave some extra details which gradually came to mind. |
|
Vignette 2: |
|
The claimant stated she had never needed to attend her GP before the index work accident (slip on wet floor) for psychological problems and had never had psychotropic medication or counselling. When shown the GP notes which illustrated a significant history of antidepressants prescribed for worked related stressors, including on disciplinary, her affect (emotionality) didn’t alter and she rationalised that this was not related to any slopping or tripping accidents. Her rationale was consistent with her having decided this information was ‘not relevant’ rather than a memory deficit. |
The following list of common types of information being omitted are: -
Information Omitted include events (similar to index); adverse life events; medical treatment (related); forensic events and medical treatment (unrelated).
1. Reasons given for omission once questioned include; lack of immediate recall (recall on prompting); lack of any recall (totally forgotten); lack of perceived relevance; embarrassment and guilt and social undesirability in context of claim.
2. Claimants’ emotional reaction to subsequent questioning include apologetic and acquiescent (and provided more information gradually); no change in affect and defensive and resentful and/or guilty
Reliability of Strategies to enhance pre-index event history given
It is of intent to the court to ensure the highest degree of reliability and truthfulness when obtaining evidence.
Two school of thought exist as to the best method of achieving this:
a) Careful assessment of claimant’s style of evidence giving including omissions or apparent ‘misunderstanding’ and expert interpretation of this, or
b) Guiding and encouraging the claimant in how to provide the best quality, highest accuracy evidence and discouraging, from the onset, any attempts to prevaricate or be selective.
The problem with (a) is that when the expert detects ambiguity, he/she is left in a quandary about to interpret this (i.e. memory factors, untruthfulness). Conversely, in (b), the claimant’s tendency towards possible untruthfulness is reduced by the expert’s advice and encouragement to ‘keep to the truth’. On balance, however, the second option is usually the more advantageous and beneficial to all parties concerned (Koch, 2015) (a).
The following strategies are highlighted as helping this process:
1. At the beginning of the interview, encourage the claimant to:
a. Keep to information that is clearly remembered
b. Not to ‘make up details’ that ‘sound right’
c. Use words that are accurate (e.g. don’t say ‘nightmares’ if you mean ‘lying awake thinking’)
d. Be willing to say ‘I can’t remember’ – this is acceptable to say
e. Do not provide any information that is incorrect
2. During the interview, when a possible ambiguity arises:
a. Think carefully and try and retrieve extra details
b. Don’t worry if a discrepancy occurs, but help to resolve this by further thinking
3. At the end of the interview:
a. Review what has been said
b. Consider if any evidence given should be altered – this is acceptable to do.
Thin or crumbling skulls?
When a claimant alleges psychological injury, pre-existing psychological injury evidence is often introduced to challenge, or validate the claimant’s case (Vallano, 2013).
The eggshell claimant rule predicts that a defendant who causes damage should be liable for all the claimant’s injuries i.e, taking the claimant as one finds him/her. This is generally used when:
1. There is a dormant or underlying condition, revealed by the index injury.
2. There is a previous condition, successfully treated, which re-emerges.
3. There is a pre-existing condition, which the defendant’s negligence makes worse.
A comprehensive psychological assessment includes an evaluation of all available information about the claimant’s pre-existing, current, and prognostic/future factors. It is important to differentiate between a claimant’s emotional distress resulting from the defendant’s negligent actions and distress which may have inevitably developed, regardless of the defendant’s role, due to their pre-existing condition.
Reviewing court cases both in the UK and North America indicates that ‘skull’ rules are not applied consistently (Iezzi et al, 2013) contributing to conflicting determination of cause and damages across the courts. There is need for operational definitions of the thin skull and crumbling skull rules and how there are effectively applied.
The characteristics of a thin skull are:
-
The claimant is considered vulnerable (from earlier history)
-
Not manifesting clinically significant symptoms or impairment
The characteristics of a crumbling skull are:
-
The claimant has experienced deteriorating health and functioning prior to the index injury, which has been accelerated by the index injury.
It is important for case law and expert assessment to: -
1. Differentiate between the subtle distinctions of a) pre-existing symptoms and b) prior personality traits or vulnerability.
2. Apply the ‘but for’ rule and ‘material contribution’ rule carefully and logically.
The defendant is responsible for the costs associated with the thin skull, and only the acceleration of the crumbling skull. The ‘but for’ test assesses what could be reliably predicted to have occurred in the index time frame if the index event had not occurred. The ‘material contribution test’ is used to apportion the cause when multiple causes are identified as having contributed to the claimant’s injuries.
Determinants of cause are often complex. The following approach is recommended to determine the relevance of pre-index injury health and function ensuring the appropriate application of the above skull rules:
1. Early vulnerability which is not symptomatically evidenced immediately prior to the index accident (i.e. preceding 6 months) involves the application of the thin skull rule. This would include previous episodes of treated depression with statistical predictions from NICE (2009) of future episodes.
2. When symptoms exist immediately prior to the index event (i.e. preceding 6 months) and are exacerbated by the index event, then the crumbling skull rule applies.
3. It is important that medico-legal expert assessors demonstrate expertise and experience in evaluating claimant histories and presentation appertaining to pre, peri and post-injury factors (Iezzi et al 2013), assisted by impartiality and concise focus on available information. It is also important that lawyers, barristers and judges have available continuing professional development opportunities addressing how psychological processes such as
Improving evidential reliability via Part 35 questions
Part 35 questioning gives all parties an opportunity to improve the reliability of expert evidence.
The most common reason for asking a question is that a Defendant is asking questions of the Claimant’s expert in order to:-
1) Highlight deficiencies in the expert’s report, whether that be a failure to comply with the requirements of Part 35 and / or the Protocol, or a failure to identify and address material entries in the medical records;
2) Clarify the expert’s views on various key issues in the case, for example causation, prognosis, or the recoverability of a certain head of loss (e.g. appropriate treatment, loss of earning, handicap on the labour market);
3) Lay the foundations for an application for one’s own expert evidence in the same field;
4) Encourage the expert to change his evidence so that it is more favourable to the Defendant (questioning party) (Katyar and Kerr (2015).
Alternatively a party may ask questions of his own expert (not strictly speaking Part 35.6 questions) in order to (a) clarify matters, (b) encourage him to support various heads of loss, (c) when the expert has changed his opinion at the joint statement stage and the discontented instructing party wishes to know why the expert has performed the volte-face prior to making an application for a replacement expert.
So, how do experts and the questioning party use this mechanism to gain greater clarity, avoid defensive criticism (by either party) and contribute to case resolution? Ten written submissions of Part 35 questions sent to eight clinical psychologists were analysed for area of enquiry, length and tone (Koch et al 2015 (b)).
The following is a non-exhaustive list of areas to explore (Katyar and Kerr, 2015); -
1) Is there a sufficiently close temporal relationship between the accident trauma and onset of symptoms?
2) Flag up the relevant part of the Claimant’s previous medical history, and highlight inaccuracies from the Claimant’s self-report of symptoms.
3) Focus on aspects of the Claimant’s clinical examination. How thorough was it. Any inconsistencies.
4) Failure to mitigate; what course the Claimant’s symptoms would have taken if he had undergone recommended treatment;
5) Whether the Claimant satisfies the Equality Act test of ‘disabled’.
Given the variability and differences in psychological diagnosis, assessment and prognosis, coupled with the adversarial process in civil litigation, the option of asking Part 35 questions continues to be a constructive process, providing it stays within the remit of clarification of the expert’s report and opinion and does not venture into a legalistic ‘fishing expedition’. It is incumbent on experts to make their reports and opinions increasingly logical and internally consistent and to address inherent areas of unreliability. The opposing lawyer can then hone his/her skills in questioning the expert.
Koch’s Postulates to enhance robust opinions
Expert opinion, one foundation of civil litigation and justice, should be based on robust reasoning. An unrelated name-sake of the author, the microbiologist, Robert Koch, formulated four criteria or postulates in 1884 designed to establish robust reasoning in a different field – microbiology. He cited key principles about the causative relationship between a microbe and a disease (Koch, 1876). This concept of ‘postulate’ was also alluded to by the famous psychotherapist, David Malan, in his seminal text ‘Individual Psychotherapy and Science of Psychodynamics’ (Malan,1979), stating robust reasoning when theorizing on valid explanations for psychological symptoms. Both these famous scientists, David Malan and Robert Koch, used the term ‘postulate’ to ‘assume or assert truths as valid premises for discussion or reasoning’.
In the field of civil litigation, expert opinion can be operationalised in terms of a number of key postulates, called Koch’s medico-legal postulates (Koch, 2015) (b_. These relate to the medico-legal contexts of pre and post-index event history, multi source evidence, diagnosis, causation, prognosis and reliability. They have been arrived at following 20 years of experience in assessment and treatment of psychological injuries (see figure 5).
|
I. A robust opinion should address diagnosis, causation and attribution, duration and prognosis. |
|
II. A robust opinion will include more than one type of evidence. An opinion based on claimant self report only may still be valid but is a ‘weak’ opinion in medico legal terms. |
|
III. The classification/diagnostic categories given in DSM 5 and ICD 10 are a part of an expert’s opinion /formulation – this systematic check of relevant criteria must be balanced by wider clinical judgment. |
|
IV. The expert’s Mental State Examination should be consistent with the claimant’s description of currently active symptoms – a clear discrepancy reduces the robustness / strength of an opinion . |
|
V. Wherever possible, GP computerized attendance records should be made available to the expert. The subsequent analysis will increase the strength or reliability of the opinion given. |
|
VI. A therapist who has already treated a claimant cannot provide an impartial or independent expert opinion on issues of diagnosis, causation or prognosis on that claimant. |
|
VII. A robust opinion should include a history of factors which could, on the balance of probabilities, affect a specific index event reaction. |
|
VIII. A robust opinion should give particular emphasis to the 12 month period prior to and post the index event, but not to the exclusion of earlier or later history. |
|
IX. In any interview where the claimant displays a high level of anger, a differential opinion should be made between normal perceived injustice and clinically significant adjustment problems which might require intervention. |
|
X. An expert opinion should incrementally increase in robustness over time with access to more data and discussion with other relevant professionals, both legal and clinical. |
|
XI. An expert’s opinion should be the ‘best fit’ professional view of all available data at that time, and should be modified , if appropriate, as and when new data becomes available. |
|
XII. When key evidence is unavailable , the expert should state that the robustness of his/her opinion is reduced as a result. |
|
XIII. It is encumbent on the expert to be impartial, independent of instructing party, and maintain as high level of logicality as possible when appraising evidence. |
|
XIV. Experts should maintain a high level of accessibility to lawyers in order to encourage rapid process and resolution of litigation. |
|
XV. Experts should understand and be sympathetic to the claimant’s experience of litigation stress, irrespective of their expert opinion on the specific case. |
|
XVI. Irrespective of the prognosis for organically mediated pain, psychologically mediated ‘overlay’ can have a positive prognosis especially with pain-related CBT therapy resulting in increased pain coping and adjustment. |
Fig. 4. Summary of Koch’s Medico-legal Postulates
Whither these postulates?
Different experts will have their own varied set of beliefs underpinning their assessment methods. My postulates, above, in my opinion, account for 75% of the variance in experts’ opinions. However, as soon as this list is published, deficiencies will be recognised and discussed, no doubt! It is essential and informative to ‘recognise the wider range of contemporary approaches to build an argument…and establish proof’ (Inglis, 2007).
However, to date, these current postulates are based on congruence of a large number of assessments carried out by a team of over thirty experts, exploring and understanding dissonance when it occurred, to assemble arguments for what constitutes robustness in opinion formulation.
Any process of suggesting postulates of universal applicability with any one field are, by nature, provisional and subject to further refinement in the light of future observation. In this particular field (personal injury/civil litigation), it is anticipated that this refinement will take place in areas of vulnerability to injury, prognosis/treatment, mitigation of loss as well as procedural areas such as joint opinion formation, deception detection and reliability/truthfulness.
Conclusions: The way forward to enhance evidential reliability
In this paper, I have discussed how civil litigation is processed in the UK and a variety of areas where reliability factors effect the quality of evidence utilised by the court. It is a crucial role of the court, its lawyers and experts to all contribute to the ‘evidential reliability’ debate in any one case litigated. Further work by experts on enhancing the reliability of their evidence is needed. This will be informed by feedback from the judiciary, lawyers and insurers on concepts, data and issues that cause ambiguity and uncertainty. I am beginning to contribute to a further examination of how the Russian system compares to the UK system developing themes already outlined by Cherepanova (2013) on grounds for compensation by the state for personal injury and Kravtsova (2013) on the concepts of ‘moral damage’ of the Russain process, elaborated by the comprehensive analysis of the civil law institution by Vasilev (2013).