In the
However I can also tell some positive facts. We have very few cases of H.I.V. infected drug users. This is not the result of the distribution of methadone, but because the percentage of intravenous use of hard dugs dropped from around 80 % in the eighties to 11% nowadays. An addicts who uses needles is seen in the addict scene as sick or stupid (and nobody likes to be called stupid). Those who still use needles are always using their own equipment and know how to clean it.
Another positive fact is that there are still therapeutic communities in The Netherlands where drug addicts can learn to lead a drug free life.
The philosophy of the original therapeutic communities for addicted persons is based on the concept of self-help and mutual help. The roots of these therapeutic communities are in Synanon, a community of former addicts founded in
The residents in a therapeutic community learn to help themselves with the help of their peers. In the early American therapeutic communities for drug addicts which used this concept, the staff consisted almost entirely of recovered addicts, often graduates of the same programs.
In
In the therapeutic community the residents learn to help themselves with the help of others. All activities are part if the therapy including cleaning of the house.
There is a clear distinction from a medical model clinic (Kooyman, 2005). In the medical model addiction is regarded as a disease. The addicted person is treated as a patient, he is not responsible for his condition. Although this view has advantages over a moral view and makes medical treatment available, it has also disadvantages.
This is especially the case when addiction is called a chronic relapsing disease.
This is not only incorrect, as has been proven by research, it also gives doctors as well as the addicted persons an excuse for failing treatments.
Long term studies of the natural history of drug addiction show, that of persons addicted to hard drugs twenty years later around 40% are abstinent.
The Dutch psychologist Prof. Gerard Schippers concluded in a study of 5 reviews based on 56 original studies with data of more than 30.000 drug abusers ( including the DARP and TOPS follow-up data) that, although there is a slow increase in the number of deaths ( ca. 20% after 20 years) there is also a steadily growing number of abstainers ( 40% after 10 to 20 years). In contrast with the maturing out theory, the percentages of abstainers, abusers and non-problematic users tend to stabilize in the 10-20 year follow-up figures (Schippers, 2006). These studies were on ex-clients of drug treatment programs.
See Figure 1.
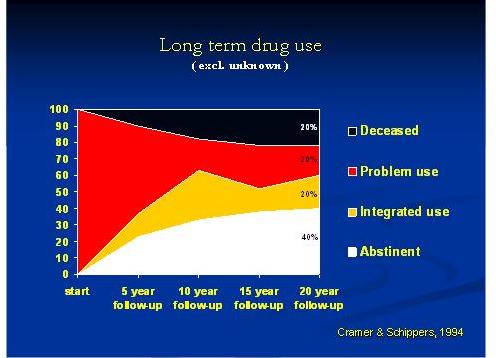
In contrast with the maturing out theory, the percentages of abstainers, abusers and non-problematic users tend to stabilize in the 10-20 year follow-up figures (Cramer and Schippers, 1994).
The studies were on ex-clients of treatment programs.
For alcohol, there are also studies in the general population., that after 18 years 39 % of the alcoholics were abstinent 18 years later.
Schippers concluded that of the people with alcohol dependency entering treatment for their alcohol problems, 60% are no longer in that condition several years later.
These findings show that chronic addiction is less common than often assumed.
Is addiction a relapsing condition?
In the review of alcohol studies, it was found that the hazard of relapse was higher in the first 4 years than after that period ( Schippers, 2006). The longer the person abstains the less likely there will be a relapse.
Harriet Barr found in a seven- year follow up of ex- residents, including all drop-outs of the Eagleville, a Therapeutic Community for drug addicts as well as alcoholics in
Therefore, we can say that a relapse does not have to occur when a person is abstinent after having been addicted to drugs and that the longer a person is abstinent the less likely he is relapsing.
Is addiction a disease?
Many doctors are now calling addiction a disease and seek for a medical solution of the addiction problem. The term disease fits in the medical model. A disease needs treatment: They do not realize, that the medical profession has been better at creating addictions than inventing a cure for them. Medication to diminish craving has so far not shown any considerable results.
In the past, addiction to opiates was treated with the prescription of heroin. Addiction to heroin was treated with the prescription of methadone.
Lifelong substitution with methadone was recommended. In the
It is only recently, that there is a growing consensus among researchers, that by life long prescribing addictive drugs such as methadone without any incentive to stop we create chronic patients.
Although addiction is often regarded as a disease, addiction is in my opinion as much a disease as fever or high blood pressure or blindness.
To call addiction a chronic relapsing disease has to be avoided as it causes unnecessary pessimism and a lack of motivation for treatment among primary care physicians (De Bruijn c.s.20005). It can become a negative self-fulfilling prophesy.
The name: chronic relapsing disease is not only incorrect, it ignores facts that are in contradiction with this name, such as the long lasting positive successes of drug free treatment.
Addiction can be better named a disorder instead of a disease, usually being a symptom of an underlying problem. Addiction can be seen as a self-inflicted disorder with multiple causes (Kooyman, 2007).There is always something else, we have to look for when a person is addicted. Addiction is a condition caused by something else, usually a combination of different factors.
The definition of addiction
The definition of addiction which follows from this is:
Addiction is a self- continuing harmful process resulting from the loss of control over adaptation behaviour which then itself becomes a problem. (Kooyman, 1992 pp. 223).
Or shorter following the Classification of the D.S.M. IV:
Addiction is a dependency disorder from which recovery is possible.
Not every person using alcohol becomes addicted. Not everybody using drugs becomes a drug addict. There must be something else within the person or in his environment
leading to addiction. Some persons are apparently more vulnerable than others. Some persons may have a genetic constitution making them more vulnerable. Some persons live in circumstances whereby there is a high risk of becoming addicted.
There is always something else, we have to look for when treating addiction.
The best way to do so is to first try to help stop the addictive behaviour, the use of the drugs that became a problem in itself and then to treat the cause.
This cause can be a co-existing mental disorder. It can also be the fear and actual pain of rejection resulting from a deprived childhood with a low self esteem as a consequence. Most residents of Therapeutic Communities were traumatized in their early childhood.
In the history of addicts we often find traumatic situations in the families which they belong to such as: incest and sexual abuse ( in female addicts we find percentages up to 90%) , suicides, the sudden death of a parent, admission to a psychiatric hospital, divorce, ( Aron, 1975 ).
Addiction is often the consequence of unresolved traumatic experiences in early childhood or later in life. The use of drugs, alcohol or medicines to alleviate the psychological pain of traumas can subsequently become a problem in itself.
When a person has become addicted he is caught in a vicious circle:" I drink because my wife is angry at me because I drink".The person is caught up in several vicious circles (van Dijk, 1971): a pharmacological vicious circle (stopping produces effects which force him to use again), a psychological vicious circle (stopping no longer hides negative thoughts or feelings such as guilt feelings which make a person use again), the vicious circle of the primary group (the friends: peers still addicted, reject a person that stops using, or the family: the addict helps the parents to stay together by being the scapegoat, presenting a problem for them, making it difficult to stop) and the vicious circle of society (the ex-addict is not trusted: " once an addict always an addict".
See Figure 2.

Treatment with abstinence as a goal has to be directed at breaking down all four circles.
This is the goal of therapeutic communities. ( Kooyman,1992).
In therapeutic communities the residents learn to solve their problems in a drug free environment with the help of their fellow residents. They learn to make mistakes without feeling themselves a failure as a person. Role models of older residents are an important element of the system as well as a clear value system. The cardinal rules are: no drugs, no alcohol, no violence or threat of violence. Breaking these rules means temporary exclusion from the Therapeutic Community. The therapy is mainly in groups.
After around one year in the therapeutic community there follows a re-entry programme, usually in a separate house, from where the residents can go to school, visit clubs, and find an occupation.
Research of therapeutic communities in different countries showed the following results:
-
approximately 30 % of all admissions never relapsed after discharge into drug abuse.
-
longer time in the program improves outcome success,
-
with a stay in the program of at least a year the success rate is more than 70%.
-
some relapse only for a short period after discharge ( 50 % of all admissions had no drug abuse or alcohol problems in the last half year of a two year follow-up in a research of the Emiliehoeve TC in The Netherlands)
-
parent participation improves successful outcome
-
treatment in therapeutic communities can be an alternative to prison.
As the length of treatment in therapeutic communities is more than a year, research following the criteria of evidence based research is difficult to implement.
However in an evidence based research in the
Therapeutic communities are successful treatment modalities for drug addicts and relatively inexpensive. Compared with other treatments for addicted persons therapeutic communities are most cost effective: The profits of the treatment are more than twice the costs of the treatment. Besides that the treatment has other benefits such as reducing the suffering of the addicts and their relatives.
Costs and benefits
The costs of a person addicted to-day to society are considerable; the costs of health care, hospitalization, incarceration, lost employment and social welfare allowances.
Treatment with abstinence as a goal means you have to invest. There are however not just costs, but also benefits. When we take in consideration the long term benefits of addiction treatment we see, that the benefits are greater than the costs. When we look at the success of treatment of addiction several measures are used such as: lasting abstinence, no illegal drug use, diminished drug use or drug free days. Other measures are: improved physical heath, prevention of infections (hepatitis, HIV) and improved liver function, improved mental health, clients satisfaction, improved social integration: no ( or diminished) crime, useful daily activities, work/education and contacts with non users. When we look at cost and benefits in health we find a reduction of the costs of treatment and additional health care and a reduction in costs of addiction treatment and general health care (doctors visits and hospitalization).
When we consider cost and benefits in crime we find no costs during in-patient treatment and as benefits of all treatment modalities reduced costs of police, justice system and prisons. Looking at work and income we find no or reduced income from work during in-patient treatment as costs and as benefits reduced social allowances during and after in-patient treatment and tax-income from work after treatment.
In a review of the literature of eighteen cost-benefit studies of various drug treatment services Cartwright, showed that a persistent finding is that benefit exceeds costs (Cartwright, 2000).
NIDA, ( the National Institute of Drug Abuse in the USA), states in its guidelines that each dollar invested in treatment results in 4 dollars reduction of crime costs and up to 10 dollars in health costs.
John Berg did a study on the benefits and costs of therapeutic communities in
James Pitts, reported at the
The savings are even greater when we look at the post treatment benefits (Pitts, 2002).
Let us see now what is the situation in the
The criteria for success were of the follow–up research of the Emiliehoeve Therapeutic Community in the Hague, the Netherlands were rather strict (after leaving the program: no use of hard drugs, only occasional use of cannabis or prescribed drugs such as sleeping pills or tranquillizers, no alcohol abuse, no treatment for addiction, no drug-related arrests or convictions and no admissions to psychiatric institutions. At the two year follow-up of the first 172 first admissions the success for all ex residents was 32 %, compared with 4,5 % for a detox-only group. It was clear that the longer the residents had stayed, the better were the results. When they stayed less than one month: 0% success, staying one year 70 % success, completions (graduates): 80 % (Kooyman, 1992). This research was repeated 10 years later with similar outcome results (van der Meer, 1997). Longer time spent in the program is related to better results.
Participation of parents in parent groups improved the success considerably. The clients who had parents attending at least two meetings had more than two times better results (Kooyman, 1992). Statistical analysis of the Emiliehoeve-data showed that this was an indirect effect: parent participation correlate with longer stay in the program what lead to a better treatment outcome. It became also apparent that some ex residents had used drugs only for a short period after discharge. When considered the last half year before the interview of the sample in the research the results showed almost half of the ex- residents being a success ( Kooyman, 1992). The successfully treated persons were no longer showing addictive behaviour. Most of them found jobs and became tax-paying citizens.
More recent promising results were found in new programs derived from the original therapeutic community in
Of the clients (92 % male) with an average age of 33 years, 28 % were more than10 years in a methadone program, 31 % had a parent born in a non western country. They had an average time spent in jail of more than four years. The main drug of 69 % was heroin with an average duration of the use of 11 years, of 19 % the main drug was cocaine with an average duration of the use of 8 years.
After nine months 50% were still in the program (average time in program: 218 days). The follow-up study one year after leaving the program showed the following results: no hard drugs ever used: 41%, there was no heroin use last month before the interview in 74% of the sample. As to social integration the following was found: employed in a job: 47 %, studying full time: 7 %. There was also a considerable reduction in crime after discharge:
It was also clear that the longer the time spent in the program the better were the results.
In The Netherlands for a limited number of heroin addicts heroin distribution programs are started some years ago. They are divided in a group that inhales the heroin and a group, that injects heroin. Both groups are also getting methadone. The only significant difference with a methadone only control group was a reduction in crime. In the injecting group the criminal behaviour (stealing, dealing) was reduced from 13 times a month to 3 times a month and in the inhaling group from 11 times a month to 3 times a month. The yearly costs are between 15.000 and 25.000 Euro per person per year. Also it was found that the persons in these programmes continued to also illegally use cocaine.
What does did mean for a cost-benefits analysis in the programmes in
The total costs for not giving any treatment at all are: 100 Euro per person per day on: social costs (social allowances , other social costs such as shelters for sleeping, drop-ins) and crime related costs (arrests, detention, prisons, court cases etc). Damage done to society through theft, burglary and other crime is not included in the figure.
Methadone maintenance or drug free therapeutic community treatments both give a daily benefit per person of 75 Euro a day to those receiving treatment.
If we look at the results after a three-year period, we can see that the profits as a result of treatment are much higher when we consider the potential success. For therapeutic communities the profit is as high as 50 Euro per client a day. The profit per person in a methadone distribution prpgramme without further treatment ( harm reduction) is zero.
The conclusion is that treatment is cost-effective and also cheaper than no treatment at all or harm reduction programs.
The psychiatrist Van der Meer did a cost-benefits analysis of the Emiliehoeve Therapeutic Community and the Triple-Ex programs. He used the analysis of the costs to society from 1997 (of the KPMG), accepted by the Council for Public Health in The Netherlands (Raad voor de Volksgezondheid). The costs for society of a hard drug addict in The Netherlands of health care, social allowances and crime are an average of 50.000
Euro a year, per person. For the addicts who are admitted to residential treatment this is a modest estimate.
For both modalities The Emiliehoeve Therapeutic Community and Triple-Ex, the total of yearly admissions is 60 for a capacity of 30 beds each. Based on the above mentioned research, we assume to discharge of these 60 persons from the Emiliehoeve 20 success cases. Assumed was a modest number of 12 persons who will stay a long term success (at least seven years) In this reswarch the total costs of treatment of a year in the Emiliehoeve, and the cost of after-care in the re-entry program were deducted by the costs saved by the successes. The total costs invested in the residents are 1.800.000 Euro. The benefits are 5.280.000 Euro. Conclusion is that the benefit-cost ratio is 2.9.
For the Triple-Ex program a similar table can be made. The benefit-cost ratio is here 2.9.
The yearly savings for each program are more 3.5 million Euros to society (van der Meer, 2002).
Conclusion
The success of the treatment in therapeutic communities is considerable.
We can attribute the following qualities to residential treatment in Therapeutic communities:
-
beds of therapeutic communities are inexpensive,
-
30 % of all admissions have a successful outcome,
-
longer time in program improves outcome success,
-
with a stay in the program of at least a year the success rate is more than 70%.
-
parent participation improves successful outcome
-
treatment can be an alternative to prison.
The financial benefits of drug addict treatment exceed the costs greatly.
This is most clear for therapeutic communities.
Investing in treatment is saving money for the society with more than a 200% profit.
Therapeutic communities are successful treatment modalities for drug addicts, if the clients can stay long enough in the program and relatively inexpensive. The benefits are greater than the costs. Besides that the treatment has other benefits such as reducing the suffering of the addicts and their relatives.