INTRODUCTION
High rates of anxiety- and depression-related disorders are well-known healthcare problems of our time. The lifetime prevalence of depression in the population is 10–15%, and is among the top three disorders leading to disability.1 The lifetime prevalence of anxiety disorders in the population is up to 33%, with anxiety-related disorders associated with high levels of impairment and excessive healthcare utilization.2 Among physical diseases, cardiovascular disease (CVD) and diabetes mellitus type 2 (DM) remain major healthcare concerns worldwide.3,4
Thus, depression, anxiety, CVD, and DM are among most prevalent health problems, and their co-occurrence can make the situation even worse. Undiagnosed depression increases the risk of mortality and cardiovascular events in patients with CVD5-7 along with a higher rate of health resource utilization;5 the same is true in patients with DM.8 Furthermore, CVD and DM are risk factors for depression.5,9,10 Anxiety is associated with poor metabolic outcomes and increased medical complications in DM,11 and with adverse cardiovascular outcomes — including death — in CVD.12 Therefore, diagnostics and treatments of anxiety and depression are an important healthcare task, especially in cases of comorbidity.
Interaction between general practitioners and mentalhealth professionals, and building an integrated primary care model, is acknowledged as being important to healthcare systems.13-15 Based on the evidence of a high prevalence of mental disorders on the one hand, and their insufficient diagnostics and treatment on the other, the WHO launched the Mental Health Gap Action Programme (mhGAP)16 in 2008 with the aim of bridging the treatment gap for people with mentalhealth problems by facilitating early detection and treatment of mental disorders. This programme is actively ongoing worldwide, with the education of medical professionals and non-medical staff considered one of the more essential steps within it.17,18
In Russia, the algorithm for diagnostics and multi-professional management of non-psychotic mental disorders in primary care settings was developed within the Federal targeted programme, the “Prevention and management of socially significant diseases (2007–2012)”, in 2010.19 Important factors that should be considered in building integrated care in Russia form the legislative and financial aspects of healthcare. Psychiatry and general medicine have different financing models, and there is a legislation barrier — Mental Health Law prevents non-psychiatrists from treating any mental health disorders themselves.20,21
The model of ongoing interaction between psychiatrists and primary care physicians (PCPhs), including the continuous education and guidance of PCPhs in dealing with patients with mentalhealth problems, was suggested and studied22 within the above Federal programme. The model required the presence of psychiatrists in primary care settings that was not, however, further implemented in routine medical practice.20
According to recent data, anxiety and depression are diagnosed 25–70 times less frequently in Russia than in other countries.23 Thus, the problem of insufficient care for patients with common mental disorders remains unsolved. To that end, timely diagnostics of mental disorders in primary care settings and referral to a psychiatrist for treatment may increase care provision to people with depression and anxiety.
The aim of this study was to explore whether the baseline rates of referrals to psychiatrists and the indicated pharmacological treatment (complying with the screening criteria) received due to depression or anxiety among patients with CVD and DM will significantly change in the primary healthcare facility after the training of PCPhs to deal with comorbid depression and anxiety (including the algorithm for referral to a psychiatrist).
METHODS
The present study was performed through two cross-sectional assessments (each on a different sample of patients) conducted before and after the PCPhs' training.
Study population
The study subjects were the consecutive patients seen by PCPhs who met the selection criteria below.
Inclusion criteria
- Adults of both sexes, 40–64 years old.
- Admitted to outpatient department to be examined by a primary care physician.
- Having one or more of the following diagnoses according to ICD-10:
◊ I10 Essential (primary) hypertension
◊ I11 Hypertensive heart disease
◊ I12 Hypertensive renal disease
◊ I13 Hypertensive heart and renal disease
◊ I15 Secondary hypertension
◊ I20 Angina pectoris
◊ I21 Acute myocardial infarction
◊ I22 Subsequent myocardial infarction
◊ I23 Certain current complications following acute myocardial infarction
◊ I24 Other acute ischaemic heart diseases
◊ I25 Chronic ischaemic heart disease
◊ Е11 Type 2 diabetes mellitus.
Instruments
Data collection
All the patients consecutively visiting PCPhs who met the inclusion criteria were evaluated for the purposes of this study. Information on sex, age, and prescribed pharmacological treatment for anxiety and/or depression was collected and entered in an electronic Case Report Form (e-CRF). Patients were asked whether they used psychopharmacotherapy and, if so, the generic name and dose of the medication was also entered in e-CRF according to the patients’ self-report. This information was related to any psychopharmacological treatment being prescribed to the patient (not only through the referral by PCPh to a psychiatrist in this study). The use of psychosocial interventions (such as psychotherapy) was not evaluated in this study.
Hospital Anxiety and Depression Scale
Additionally, patients completed the Hospital Anxiety and Depression Scale (HADS)24 in an application developed for portable devices (tablets) specially for this study. HADS is a self-report questionnaire designed to screen for anxiety and depression in primary care settings. It consists of seven questions about anxiety and seven questions about depression symptoms during the two weeks prior to completing the questionnaire. Each question has four possible answers that reflect different severities of symptoms, if present, where the minimum score of 0 means no symptoms, and the maximum score of 3 indicates pronounced symptoms. The scores for anxiety and depression are calculated separately, therefore providing the two scores reflecting the levels of anxiety (HADS-A) and depression (HADS-D). The following cut-off scores are recommended: a score of 0–7 indicates normal levels of depression anxiety; a score of 8–10 indicates borderline abnormal levels of depression anxiety; and a score of >10 indicates abnormal levels of depression anxiety.
Evaluation of psychopharmacological treatment received by patients
Patient data (from e-CRF) was assessed by an independent expert (psychiatrist). The expert completed the treatment evaluation form in the e-CRF by marking “yes” if the treatment complied with the following criteria (and “no” if this was not the case):
HADS-A and/or HADS-D <8, absence of antidepressant/anti-anxiety medication — YES
HADS-A and/or HADS-D 8–10, absence of antidepressant/anti-anxiety medication — YES
HADS-A and/or HADS-D >10, antidepressant prescribed — YES
HADS-A >10 tranquilizers prescribed — YES
*The off-label use of phenobarbital was noted in some of the patients in the sample, and this was marked with “NO”
The indicated evaluation criteria were based on the World Federation of Societies of Biological Psychiatry Guidelines for Biological Treatment of Unipolar Depressive Disorders.25 It was assumed that patients with HADS <8 did not have anxiety or depressive disorder, and therefore that pharmacological treatment would not be needed. Patients with HADS-A in the range of 8–10 may have mild anxiety that, pharmacologically speaking, could be straightforwardly managed by tranquilizers. Patients with HADS-D in the range of 8–10 may have mild depression that would not otherwise need pharmacological treatment. For HADS >10, it was assumed that patients have anxiety or depressive disorder that requires pharmacological treatment. The prescription of herbs was included as a pharmacological treatment, but was not relevant for the treatment indication criteria mentioned above, since it is not included in the treatment guidelines25 (except for the St. John's Wort, which would be relevant but was not present in the treatment of the study participants).
Study stages and procedures
The stages and procedures of the study are presented in Figure 1.
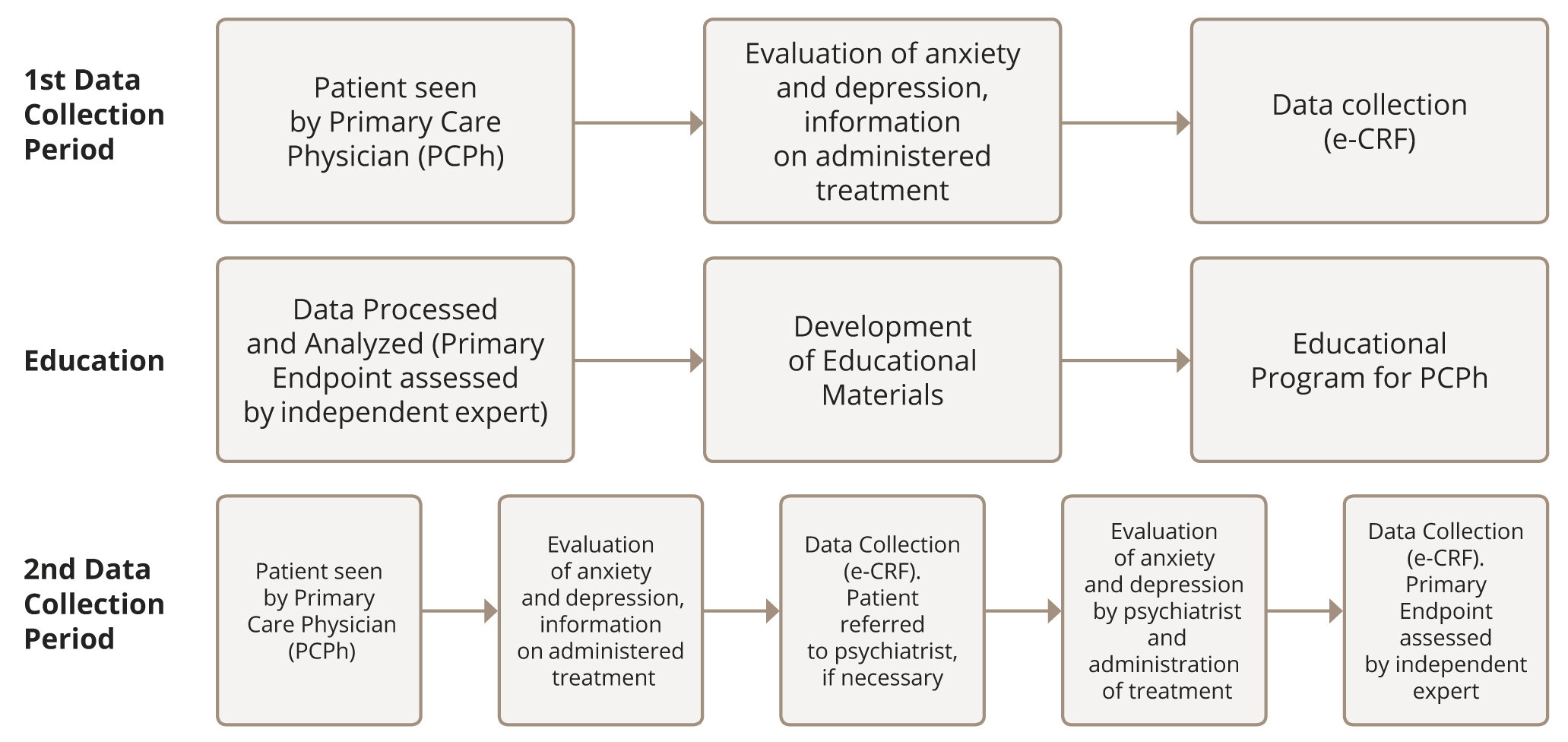
Рисунок 1. Схема процедуры исследования.
Stage 1 — 1st Data Collection (6.08.2020–8.10.2020)
Sample 1 was recruited as consecutive patients who met the mentioned inclusion criteria. They completed the HADS, and their e-CRF data was collected as described above. The indicated pharmacological treatment for depression or anxiety was entered in the patient’s record, if present. All referrals to other specialists were performed as usual (based on the PCPh’s clinical evaluation).
Stage 2 — training of PCPhs and changing the pattern of clinical care
After analysing the data obtained at Stage 1, Stage 2 of the study was initiated. PCPhs who assessed the patients in Stage 1 passed the training on clinical diagnostics of anxiety and depression, including the instruction to use HADS as a screening tool to detect patients who needed further evaluation for depression and anxiety. A new referral model for patients with abnormal HADS scores was proposed. PCPhs were instructed to refer patients with anxiety (HADS-A) and/or depression (HADS-D) score >7 to a psychiatrist in the local mental health dispensary (specialized outpatient mental facility). Referrals could be performed either by advice to visit a psychiatrist or by prescription for a psychiatric consultation on the referral blank, depending on the local referral procedures in the primary care facility.
In the training module, the results of Stage 1 were presented to the PCPhs to make them aware of the level of anxiety and depression among their patients. Training included information about the diagnostic criteria of anxiety and depressive disorders, and evidence of the advantages of treatment for patients with abnormal levels of anxiety and depression, both for their mental state and for the successful treatment of CVD and DM. Training included basic communication strategies while speaking about mental health with the patient and motivation technics that could be used in the discussion of the need to treat mental disorders and visit psychiatrists. These were intended to help the PCPhs to start dialogues with their patients about mental health and to encourage them to make appropriate referrals to psychiatrists.
Training was performed in the form of a three-hour lecture that was supplied with an educational video on how to diagnose mental health problems in a primary care setting and on the communication skills needed to discuss these issues with the patient. Motivational techniques for referral to psychiatrics were provided in the video lesson, whilst the referral algorithm was also discussed during the lecture.
Stage 3 — 2nd Data Collection (27.01.2021–18.04.2021)
Sample 2 was recruited by the PCPhs involved in Stage 1 and Stage 2 from consecutive patients meeting the inclusion criteria. All information was assessed as per Stage 1.
Setting
The Consultative Diagnostic Polyclinic #121 of the Moscow Healthcare Department.
Participants
During the first data collection period, the data on 400 patients was collected (Sample 1), whilst during the second data collection period, data was collected on 178 patients (Sample 2).
The associated sample characteristics are presented in Table 1.
Table 1. Patients’ demography and HADS scores in the study samples
|
Sample 1 |
Sample 2 |
|
|
n |
400 |
178 |
|
male |
112 (28.0%) |
37 (20.8%) |
|
female |
288 (72.0%) |
141 (79.2%) |
|
age (Mean (SD; SE)) |
55.8 (5.7; 0.3) |
55.6 (6.2; 0.5) |
|
HADS-D Scores |
||
|
0–7 scores — normal |
84 (21.0%) |
39 (21.9%) |
|
8–10 scores — borderline abnormal |
206 (51.5%) |
88 (49.4%) |
|
11–21 scores — abnormal |
110 (27.5%) |
51 (28.7%) |
|
HADS-A Scores |
||
|
0–7 scores — normal |
196 (49.0%) |
53 (29.8%) |
|
8–10 scores — borderline abnormal |
142 (35.5%) |
61 (34.3%) |
|
11–21 scores — abnormal |
62 (15.5%) |
64 (36.0%) |
Statistical analysis
Descriptive statistics were used for data analysis. Continuous data were presented according to mean, standard deviation, median, and range. Discrete data were presented with absolute and relative frequencies (percentage). The equivalence of the two proportions was tested via a two-sided z-test, whilst differences in frequencies between two groups were tested via a two-sided χ2-test using standard R language libraries at a significance level of 95%.
Ethical approval
The study was approved by the Independent Interdisciplinary Ethics Committee on Ethical Review for Clinical Studies (protocol No. 05, 13.03.2020). All patients signed an informed consent form before participation in the study.
RESULTS
Patients who screened positive (>7) on any or both of the HADS scales were comparably represented in both samples: 365 (91.2%) for Sample 1 versus 164 (92.1%) for Sample 2, (χ2=0.124 p=0.72). Distribution between HADS-D scores was comparable in both samples, whereas the distribution of HADS-A scores differed between the samples. Sample 2 had a significantly higher number of patients with abnormal HADS-A scores (>10) (χ2=30.2; p <0.0001), and a significantly lower number of normal scores (HADS 0–7) (χ2=18.6; p <0.0001).
Table 2. HADS scores and diagnoses of patients in the samples
|
Diagnoses |
Sample 1 |
Sample 2 |
||||
|
Total |
HADS-A and/or HADS-D<7 |
HADS-A and/or HADS-D>7 |
Total |
HADS-A and/or HADS-D<7 |
HADS-A and/or HADS-D>7 |
|
|
n |
400 |
35 |
365 |
178 |
14 |
164 |
|
I10 Essential (primary) hypertension |
84 (21.0%)** |
7 (20.0%) |
77 (21.1%)** |
14 (7.9%)** |
0 (0.0%) |
14 (8.5%)** |
|
I11 Hypertensive heart disease |
316 (79.0%)* |
28 (80.0%) |
288 (78.9%)* |
154 (86.5%)* |
12 (85.7%) |
142 (86.6%)* |
|
I12 Hypertensive renal disease |
11 (2.8%) |
0 (0.0%) |
11 (3.0%) |
1 (0.6%) |
0 (0.0%) |
1 (0.6%) |
|
I13 Hypertensive heart and renal disease |
15 (3.8%) |
0 (0.0%) |
15 (4.1%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
|
I15 Secondary hypertension |
9 (2.3%) |
0 (0.0%) |
9 (2.5%) |
1 (0.6%) |
0 (0.0%) |
1 (0.6%) |
|
I20 Angina pectoris |
42 (10.5%) |
4 (11.4%) |
38 (10.4%) |
14 (7.9%) |
3 (21.4%) |
11 (6.7%) |
|
I21 Acute myocardial infarction |
11 (2.8%) |
0 (0.0%) |
11 (3.0%) |
4 (2.2%) |
1 (7.1%) |
3 (1.8%) |
|
I22 Subsequent myocardial infarction |
5 (1.3%) |
0 (0.0%) |
5 (1.4%) |
1 (0.6%) |
0 (0.0%) |
1 (0.6%) |
|
I23 Certain current complications following acute myocardial infarction |
5 (1.3%) |
0 (0.0%) |
5 (1.4%) |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
|
I24 Other acute ischaemic heart diseases |
19 (4.8%) |
2 (5.7%) |
17(4.7 %) |
2 (1.1%) |
0 (0.0%) |
2 (1.2%) |
|
I25 Chronic ischaemic heart disease |
50 (12.5%) |
6 (17.1%) |
44 (12.1%) |
28 (15.7%) |
5 (35.7%) |
23 (14.0%) |
|
Е11 Type 2 diabetes mellitus |
100 (25.0%) |
7 (20.0%) |
93 (25.5%) |
33 (18.5%) |
1 (7.1%) |
32 (19.5%) |
* p <0.05, **p <0.001
The distribution of positive HADS scores depending on CVD and DM diagnoses of patients are presented in Table 2 for both samples. The number of patients with diagnosis I10 Essential (primary) hypertension was significantly lower in Sample 2 compared with Sample 1 (χ2=15.1; p=0.0001), as was the number of patients with positive HADS scores (>7) (χ2=12.5; p=0.0004). The number of patients with diagnosis I11 Hypertensive heart disease was significantly higher in Sample 2 compared to Sample 1 (χ2=4.6; p=0.03), as was the number of patients with positive HADS scores (>7) (χ2=4.4; p=0.04). Other differences between the two samples were not found to be statistically significant.
The number of patients with the prescribed psychopharmacological treatment and the number of patients where this treatment was indicated according to the study criteria upon the expert evaluation for both samples are presented in Table 3.
Table 3. Prescribed pharmacological treatment for anxiety and depression and its indication according to the study criteria
|
Sample 1 |
Sample 2 |
|||||
|
Total |
HADS <7 |
HADS >7 |
Total |
HADS <7 |
HADS >7 |
|
|
Psychopharmacological treatment prescribed |
||||||
|
n |
400 |
35 |
365 |
178 |
14 |
164 |
|
yes |
119 (29.8%) |
9 (25.7%) |
110 (30.1%) |
59 (33.1%) |
3 (21.4%) |
56 (34.1%) |
|
Psychopharmacological treatment indicated by the study criteria |
||||||
|
n |
119 |
9 |
110 |
59 |
3 |
56 |
|
yes |
46 (38.7%) |
7 (77.8%) |
39 (35.5%) |
14 (23.7%) |
2 (66.7%) |
12 (21.4%) |
Although it was expected that patients from Sample 2 with a HADS-A/HADS-D >7 would be referred to a psychiatrist for diagnostics and treatment prescription or correction, no one from Sample 2 actually met the psychiatrist through the PCPhs' referrals.
There was no significant difference between samples in terms of the proportion of patients who received the indicated pharmacological treatment according to the study criteria (χ2=2.8; p=0.09).
DISCUSSION
The results of the study revealed a high proportion of patients with CVD and DM having HADS-A and/or HADS-D scores >7 in both study samples (91.2% and 92.1%, respectively). One-third of the patients with the positively screened HADS scores received psychopharmacological treatment, but only in 21.4%– 35.5% cases was the treatment indicated in compliance with the screening criteria used in this study. The training of PCPhs did not seem to affect the pattern of delivery of care offered to the patients in Sample 2 — no one in this sample received a consultation with a psychiatrist through a PCPh referral, nor received the indicated pharmacological treatment to any greater extent than the patients in Sample 1.
The level of positively screened (borderline or abnormal) anxiety and/or depression according to HADS (>7) reveled by our study exceeds the known rates of in CVD observed in other studies that used the same screening tool (47.2% for anxiety and 42.5% for depression).26 The level of abnormal anxiety and/or depression according to HADS (>10) revealed by our study also differs from the known data.27 Our results may partly be explained by the fact that our study was performed during the COVID-19 pandemic. On the one hand, the pandemic was a stressor that could have increased levels of anxiety and depression among patients; on the other, only those patients with more pronounced health problems would have been seeking medical help during the pandemic.28 This may explain why in our study depression, according to HADS, was more frequent than anxiety, whereas in the mentioned studies anxiety was more frequent than depression.26,27
When it comes to the number of the patients who received the indicated pharmacological treatment for probably having anxiety and depressive disorder in our study, this corresponds with known data from previous studies on the treatment of depression in primary care.14,29
The fact that patients did not meet the psychiatrists through PCPh referral after PCPhs were trained to detect depression and anxiety and to perform referrals may be due to several reasons. First, the brief education provided might not have been sufficient to change their patterns of care delivery. More interactive training may be needed, with feedback on how much the PCPhs have actually understood the concepts, and how much they have developed the skills needed for the implementation of the proposed protocols. Furthermore, their learning achievement may have to be continuously monitored, and may require more time for the implementation of knowledge and the change to be visible. Second, the segregation of mental health and general medicine services that leads to organizational difficulties in referrals and territorial separation of community mental health facilities (dispensaries) from primary care facility may add to the risk of patients’ non-compliance with the PCPhs’ recommendations to visit a psychiatrist. Finally, patients’ and physicians’ stigma-related fears may be a serious barrier to getting a psychiatric consultation.30
The effect of PCPhs’ mental health training is studied within the WHO mhGAP initiative in low-to-middle income countries,31 and the number of referrals to specialized care is one of the estimated outcomes in some studies.32,33 Interestingly, referrals of patients with mental health problems from primary to specialized care is seen as an undesirable effect of training, since it is associated with a reduction in PCPhs’ capacity to deal with psychiatric disorders, reduced knowledge, work experience, and poorer attitude towards mental health problems,32,34 contrary to hospital settings where referrals to psychiatrist are welcomed.35 In our study, the referral to a psychiatrist in primary care settings would be seen as a desirable effect of PCPhs' training, taking into consideration the Russian healthcare system’s particular features such as restrictions on non-psychiatrists being allowed to treat mental disorders. Therefore, the differences in healthcare systems between the countries may make it difficult to make direct international comparisons of the study results.
Our research has several limitations. First, the assumptions of the presence of depression and/or anxiety and judgments on the pharmacological treatment being correctly indicated were based solely on the HADS score which, even though it is a valid screening tool, is not a substitute for clinical diagnostics and assessment. Second, the study was performed during the COVID-19 pandemic, a major unpredicted confounding factor that changed overall patterns of care delivery in primary care settings. This extraordinary situation led to physicians being overloaded with work, significant changes in patient flows, and reduced availability of non-urgent medical care.36,37 Working conditions during the pandemic could have influenced doctors’ ability to acquire the new skill of patient referral to psychiatrists that, even in more normal situations, would meet considerable resistance due to stigma-related issues.38,39 Third, the information about psychopharmacological treatment was collected according to the patients’ self-reports, and was limited purely to the drug name and dose, with no mental health history collected. Fourth, no information on psychosocial treatments that patients may have had (supportive counseling, individual or group psychotherapy, etc.) were collected during the study, and these procedures may have affected the further need for pharmacological treatment, since contemporary guidelines suggest that for mild to moderate cases of depression, psychosocial intervention should be used as the first line of treatment.40,41
In spite of these limitations, this study did have several advantages. It is the first study to our knowledge whose aim was to assess the effect of training of PCPhs with straightforward instructions and guidelines to perform patient referrals for those who screened positively for depression and anxiety to a psychiatrist. Furthermore, this study was performed in naturalistic primary care settings, and all study procedures were adjusted to the routine working conditions of PCPhs. In addition, the specifics of the Russian healthcare system, with the need to refer all patients with suspected mental health problems to psychiatrists, was considered.
CONCLUSION
The study revealed high levels of anxiety and depression in patients with CVD and DM undergoing treatment in primary care facilities, and a lack of the prescribed indicated pharmacological treatments for these conditions. Barriers to referrals for consultation with psychiatrists do exist, despite PCPhs’ focused training and an otherwise straightforward referral protocol.
The study results indicated several requirements for primary care practice and healthcare. The high levels of depression and anxiety in patients with CVD and DM revealed by the screening in a primary care setting may point to the need for more careful diagnostics of anxiety and depression disorders in routine primary care. The brief training that the PCPhs received may not be sufficient to make a difference in healthcare delivery patterns, implying the need for more profound training of physicians in the diagnostics and treatment of common mental disorders and, indeed, in motivating patients to visit mental health professionals. The physicians’ skills acquisition may have to be monitored and evaluated on an ongoing basis, with problem-solving interventions provided where needed. More research is needed to identify and evaluate the most efficient ways to train physicians in the early recognition of and intervention related to anxiety and depression among patients with CVD and DM. Furthermore, closer interactions between mental health professionals and PCPh may be needed to overcome the barriers to referring patients with mental health problems to psychiatrists. Finally, more research is needed to identify the barriers in receiving treatment in specialized community mental health settings for patients and in physicians making referrals.