INTRODUCTION
A significant number of patients with schizophrenia experience symptoms of depression [1–5]. Depression has been observed in 20% of patients with schizophrenia during remission, while its incidence increases to 60% during acute episodes. The incidence of depression can reach 80% based on medical history, particularly in the early stages of schizophrenia [6]. Depression is one of the main symptoms of schizophrenia and one of the diagnostic signs of schizophrenia spectrum disorders [5–7]. This does not contradict the traditional division drawn between affective disorders and schizophrenia. An intermediate diagnostic category of schizoaffective psychosis defines the concept of phenotypes with a different representation of psychotic and affective disorders, or a multidimensional phenomenological continuum from conditionally “pure” schizophrenia to “pure” bipolar disorder [8–10]. The remaining challenge is determining the key features that allow one to distinguish between intermediate forms of psychotic and affective disorders. For example, symptoms of depression in patients with schizophrenia are associated with cognitive impairment. These symptoms are difficult to distinguish from the typical negative symptoms of schizophrenia in real-world clinical practice. Differential diagnosis is difficult, because signs of irreversible negative symptoms are similar to signs of depression, even in definite and long-term schizophrenia [1, 5, 11, 12]. Difficulties in the differential diagnosis between affective disorders or negative symptoms are common in the presence of symptoms such as anhedonia, mental anesthesia, emotional indifference, loss of motivation, anergy, flat affect, social withdrawal, ideational retardation, and impoverished thinking [1, 6, 11, 13]. Sometimes it is difficult to immediately distinguish between depression and catatonia [14, 15]. Notably, severe depression might be associated with psychotic features, such as delusions, hallucinations, and conceptual disorganization [1]. Sometimes, symptoms of depression are obvious signs of established schizophrenia. Even in such cases, there is the problem of determining the role of depression in the structure of the psychopathological syndrome, determining its influence on the course of the disease, its role as a target of therapy, and the complications [13, 16]. Treatment for depression associated with schizophrenia usually includes various combinations of antipsychotics, mood stabilizers, and antidepressants. However, this approach is controversial and associated with polypharmacy [13, 16–22]. This combined treatment has both desirable and adverse effects [19, 22]. The combination and severity of both affective and psychotic symptoms in a patient with schizophrenia should inform the selection of pharmacological treatment. An ideal treatment should affect depressive, positive, and negative symptoms, and it should carry minimal risk of complications. Drugs that combine the properties of antipsychotics and antidepressants due to the polyvalence of neurochemical activity appear promising [4, 13, 21, 23]. Lurasidone (Latuda®) demonstrates such properties, and it possesses selectivity for and high affinity to dopamine D2 receptors [24–26], partial agonism to 5-HT1А, antagonism to 5-HT2А, and antagonism to the 5-HT7 subtype of serotonin receptors [24, 27]. It also demonstrates selective antagonism to the α2С subtype adrenergic receptors in the prefrontal cortex [27]. Strong selective D2 receptor antagonism provides a reliable antipsychotic effect with minimal involvement of dopamine transmission in the prefrontal cortex and associated minimal effects on cognitive functions, while a complex effect on the serotonergic system provides much more diverse clinical effects of the drug. Thus, partial agonism to 5-HT1А and blockade of 5-HT2А increase the dopamine level in the prefrontal cortex and reduce the cognitive and negative impairments associated with schizophrenia. Lurasidone also normalizes the dopamine levels in the nigrostriatal and tuberoinfundibular pathways, which reduces the risk of extrapyramidal symptoms and neuroleptic depression [25, 28]. The incidence of hyperprolactinemia was comparable to the placebo [29]. Due to the blockade of 5-HT7 receptors, lurasidone possesses antidepressant and anxiolytic properties, normalizes circadian rhythms and sleep quality, improves memory, concentration, and cognition, reduces pain sensitivity, and even possesses an antipsychotic effect [27, 28]. Lurasidone increases the release of norepinephrine and, thereby, contributes to its antidepressant effect by blocking presynaptic and autoregulatory α2С adrenergic receptors [27]. At the same time, it has no appreciable affinity for the M cholinergic, α1 adrenergic, 5-HT2С serotonin, or histamine H1 receptors, which are “undesirable” receptor targets. Thus, lurasidone rarely causes such adverse events as paresis of accommodation, urinary retention, cognitive and memory impairment, tachycardia and orthostatic hypotension, QT prolongation, metabolic disorders, drowsiness, increased appetite, and weight gain [24, 25, 27–29]. Moreover, patients previously treated with some other second-generation antipsychotics have experienced weight loss within a year of switching to lurasidone therapy [30, 31]. In general, a positive impact on body weight, metabolism, and prolactin levels has been noted after a switch to lurasidone. It possesses a very low probability of drug-drug interaction [32]. Lurasidone is overall well-tolerated by patients, and it could be used in the presence of various comorbid mental conditions. Lurasidone has been established as a drug of choice in patients with metabolic disorders and cardiovascular risks [32].
Lurasidone is effective in the treatment of acute psychotic symptoms, as has been demonstrated by a number of RCTs. Its efficacy is similar to that of other second-generation antipsychotics [29, 33–36]. Lurasidone robustly reduces the scores of Marder PANSS factors [37] of positive symptoms and arousal/aggression. At the same time, significant improvement is also evident on all other PANSS parameters, including anxiety/depression, as well as cognitive impairment/disorganization [38]. While on lurasidone, patients have reported greater awareness of their illness and have been more compliant with treatment [39]. The effectiveness of the drug at reducing symptoms of depression was also confirmed using MADRS [35] and HDRS-21 [40]. Lurasidone has demonstrated a long-term relapse-prevention antidepressant effect [36]. Patients taking lurasidone have a higher level of compliance and lower discontinuation rates compared to patients taking other atypical antipsychotics [32, 41]. Lurasidone has demonstrated efficacy in acute bipolar depression, both as monotherapy [42] and in combination with mood stabilizers [43]. Studies showed relief of depression and anxiety, as well as cognitive and quality-of-life improvement. It is important that the incidence of affective phase inversion of bipolar disorder was the same as with the placebo. Therefore, lurasidone presents valuable treatment options for bipolar disorder [42, 43]. Lurasidone proved superior to placebo in terms of the effects on depressive symptoms during the acute phase of schizophrenia according to the pooled RCT analysis. Moreover, the antidepressant effect does not depend on the antipsychotic effect [35, 40, 44]. The data support the inclusion of lurasidone in the treatment of depressive symptoms in patients with schizophrenia [44]. Thus, lurasidone possesses a wide range of non-dopamine receptor activities, which determine its antidepressant and pro-cognitive effect, along with its impact on negative symptoms. Lurasidone represents an alternative to routine treatment where patients with schizophrenia and depressive symptoms are given an antipsychotic along with an antidepressant. However, the effectiveness of lurasidone in exacerbations of schizophrenia, including psychotic and depressive symptoms in a real-world setting, requires additional research.
The objective of this study was to evaluate the effectiveness of lurasidone 40–160 mg per day for the treatment of an acute episode of schizophrenia associated with depressive symptoms in real-world clinical practice in the Russian patient population.
The objectives of the observational program included:
- assessing symptoms of schizophrenia using the Positive and Negative Syndrome Scale (PANSS);
- assessing depressive symptoms using the Calgary Depression Symptoms Scale (CDSS); and
- evaluating lurasidone safety and tolerability.
The primary endpoint was to achieve a decrease in depressive symptoms consistent with the Minimum Clinically Important Difference (MCID), characterized by a decline of at least 1.3 points according to the CDSS [45]. A secondary endpoint was a reduction in the severity of schizophrenia symptoms, as measured by PANSS and its subscales (positive and negative symptoms and general psychopathology).
METHODS
Study design
A prospective observational cohort study of patients with acute exacerbation of schizophrenia, concomitant with depressive symptoms, was conducted in Russian specialized research institutes and health care facilities: Mental Health Research Center and Psychiatric Hospital No. 1 named after N.A. Alexeev (Moscow), Psychiatric Hospital No. 1 named after P.P. Kashchenko, City Psychiatric Hospital No. 3 named after I.I. Skvortsov-Stepanov and City Psychiatric Hospital No. 6 (St. Petersburg), Republican Clinical Psychiatric Hospital, Republic of Bashkortostan (Ufa), Stavropol Regional Clinical Psychiatric Hospital No. 1 (Stavropol), and the Volgograd Regional Psychiatric Hospital (Volgograd). The study sample consisted of men and women with confirmed diagnoses of schizophrenia (per DSM-V-TR) and concomitant depressive symptoms who were prescribed lurasidone at a dose of 40–160 mg per day.
Inclusion criteria:
- written informed consent for the collection and anonymized processing of socio-demographic, medical, and psychometric data;
- paranoid schizophrenia (F20) diagnosed according to ICD-10, including F20.00 — continuous course; F20.01 — episodic course with a progressive defect; F20.02 — episodic course with a stable defect; F20.03 — episodic relapsing (recurrent) current F20.09 — follow-up period of less than a year;
- schizophrenia exacerbation which required a change in a health care setting (treatment in psychiatric hospital or outpatient hospital), changes in antipsychotic therapy, and second-generation antipsychotics prescription; exacerbation included psychotic symptoms and the onset or worsening of depressive symptoms requiring pharmacological intervention as judged by the treating physician;
- moderate or severe exacerbation: a total PANSS score of at least 70 and a total CDSS score of at least 6;
- lurasidone prescription (treating physician prescribes lurasidone regardless of the program design and the objective of the study); and
- aged between 18 and 65 years old.
Exclusion criteria:
- refusal or lack of capacity to comply with study evaluation;
- participation in another clinical study;
- lurasidone contraindications which were determined by the physician according to the clinical signs of the disease, concomitant diseases, and other individual risks, as well as contraindications specified in the instructions for use approved by the Ministry of Health of the Russian Federation.
All patients received lurasidone orally once or twice daily as clinically appropriate and indicated by current clinical guidelines in the Russian Federation. The primary treating physicians determined the treatment regimen based on the individual needs of each patient; the physicians were not influenced by the objectives of the study. Patients could receive concomitant medications (i.e., mood stabilizers, sedatives, hypnotics, etc.) as clinically indicated.
Premature cessation of follow-up occurred after discontinuation of lurasidone for any reason, such as when the physician changed the antipsychotic or prescribed a second antipsychotic with a strong selective antipsychotic effect, when lurasidone was not effective against depressive symptoms and an antidepressant had to be prescribed, or when the physician or patient had decided to discontinue follow-up in the best interests of the patient.
The study was conducted from December 2020 to September 2021. Study evaluations were done before the start of treatment, on Day 1 and then on Days 4, 7, 14, 28, and 42 with an allowable interval of ±1 day. The maximum follow-up period for each patient was six weeks. We developed a special individual registration card that included anonymous data on the age, locality, diagnosis, additional therapies, the presence or absence of adverse events, and predominant symptoms and their severity. We recorded the onset, completion, or discontinuation of the study, indicating the reasons for the latter.
Evaluation tools
Psychotic and depressive symptoms were quantified using special scales, such as:
1) The Calgary Depression Scale for Schizophrenia (CDSS) [46], which is a nine-item scale where each item is scored from 0 to 3. The scale showed high internal and interrater reliability in assessing the depressive symptoms associated with schizophrenia [46].
2) Positive and Negative Syndrome Scale (PANSS), which typologically and multidimensionally evaluates psychopathological symptoms [47].
The study group included 168 patients aged 18 to 65 with a diagnosis of paranoid schizophrenia according to ICD-10. All of them were treated in an inpatient facility or day hospital for schizophrenia exacerbation, accompanied by depressive symptoms at the time of the study onset. One hundred forty one patients (83.9%) completed the observational program and made seven visits.
Statistical analysis
The general characteristics of the population are processed using descriptive statistics. Continuous variables are presented as mean values, standard deviations (SD), medians, and first and third quartiles (Q1 and Q3). Qualitative variables are presented as frequencies and percentages. Mean values were compared between the groups using a one-way analysis of variance (One-way ANOVA), and the distribution of categorical variables using Fisher’s exact test. Data were analyzed according to the PANSS positive (P1–P7), negative symptoms (N1–N7), and general psychopathology (G1–G16) subscale scores, PANSS total score, CDSS total score, and time to study completion. The significance of score changes on the scales was assessed via a dispersion analysis for repeated measurements (single-factor or multi-factor, depending on the comparison type). We also assessed changes in scale scores during each visit between groups. The study calculated the differences between Visit 1 and Visit n, which were then entered into a two-way ANOVA to compare groups. Post-hoc comparisons took into account the appropriate correction for multiple comparisons according to Dunnett’s test for duplicate values and Tukey’s test for between-group contrasts, when necessary.
We calculated the average and total doses of lurasidone for each patient and then determined the total drug exposure and the individual dose range (40–80, 120, or 160 mg per day).
Time to study completion was evaluated using the Kaplan-Meier survival analysis.
All analyses were performed using the GraphPad software (GraphPad Prism version 9.3.1 for Windows, GraphPad Software, San Diego, California USA, www.graphpad.com), except for the survival analysis, which was done using the NCSS software (NCSS 2021 Statistical Software (2021). NCSS, LLC. Kaysville, Utah, USA, ncss.com/software/ncss.)
The analysis included all patients, even those who dropped out of the study prematurely. The last-observation-carried-forward (LOCF) approach was used for the patients who dropped out of the study prematurely.
RESULTS
All study patients displayed various forms of paranoid schizophrenia at the start of the treatment for their then-exacerbation in a psychiatric hospital. The mean age of the men and women did not differ significantly. The main psychopathological syndromes at the start of the follow-up were affective-delusional, including depressive-paranoid (n=95), hallucinatory-paranoid (n=44), depressive or anxious-depressive (n=28), and catatonic (n=1). All patients experienced depressive symptoms of varying severities.
Table 1 shows descriptive sample statistics.
Table 1. Clinical and demographic characteristics of the studied group of patients
|
Gender |
Females (N=112) |
Males (N=56) |
Total (N=168) |
Test statistics |
|
Age 1 |
F=0.095, df=1, p=0.758 |
|||
|
Mean (SD) |
31.667 (11.168) |
31.125 (9.701) |
31.485 (10.672) |
|
|
Median (Q1, Q3) |
30 (23, 37) |
31 (25, 38.25) |
31 (23, 37.5) |
|
|
First psychotic episode 2 |
p=0.032 |
|||
|
No |
58 (51.8%) |
33 (58.9%) |
91 (54.2%) |
|
|
Yes |
19 (17.0%) |
3 (5.4%) |
22 (13.1%) |
|
|
Missed |
35 (31.2%) |
20 (35.7%) |
55 (32.7%) |
|
|
Age of first psychotic episode 1 |
F=3.831, df=1, p=0.053 |
|||
|
Missed |
35 |
20 |
55 |
|
|
Mean (SD) |
18.260 (12.444) |
22.750 (8.554) |
19.690 (11.505) |
|
|
Median (Q1, Q3) |
20 (15, 24) |
21.5 (18.75, 26.25) |
20 (18, 25) |
|
|
Hospitalization Number 1 |
F=4.235, df=1, p=0.041 |
|||
|
Missed |
2 |
1 |
3 |
|
|
Mean (SD) |
2.600 (1.978) |
3.327 (2.435) |
2.842 (2.161) |
|
|
Median (Q1, Q3) |
2 (1, 3) |
3 (2, 4) |
2 (1, 4) |
|
Note: 1 One-way ANOVA, 2 Fisher exact test. Statistical test are provided for non-missed comparisons between males and females.
Primary and secondary lurasidone effectiveness endpoints
The primary lurasidone effectiveness endpoint in the study was the comparison of the changes in the total CDSS score over the study period. Secondary endpoints were the changes in the total PANSS and positive, negative, and general psychopathology subscale scores in the comparison. Table 2 shows the ANOVA results for repeated measurement of the evaluation parameters; the independent factor is the visit number. Table 3 and Figure 1 show details of the means compared to Visit 1 according to a post-hoc analysis with Dunnett’s test correction. All effectiveness parameters demonstrated a significant visit effect, according to partial eta-squared values ranging from 0.39 to 0.59, reflecting the large impact of size (CDSS ηp2=0.48, PANSS, positive subscale ηp2=0.55, PANSS, negative subscale ηp2=0.53, PANSS, general psychopathology subscale ηp2=0.39, PANSS total score ηp2=0.59) (Table 2). The mean (95% CI) reduction in the total CDSS score at Visit 5 compared to Visit 1 was 7.000 [5.72–8.28] points (t(167)=13.49, p <0.001). Mean changes in the positive, negative, and general psychopathology subscales, as well as the total PANSS score, were 9.02 [7.61–10.44] (t(167)=15.74, p <0.001), 7.98 [6.62–9.33] (t(167)=14.54, p <0.001), 1.77 [14.00–22.71] (t(167)=10.40, p <0.001) and 38.14 [32.32–43.95] (t(167)=16.16, p <0.001), respectively (Table 3). Each effectiveness parameter at Visit 1 showed statistical differences starting from Visit 2.
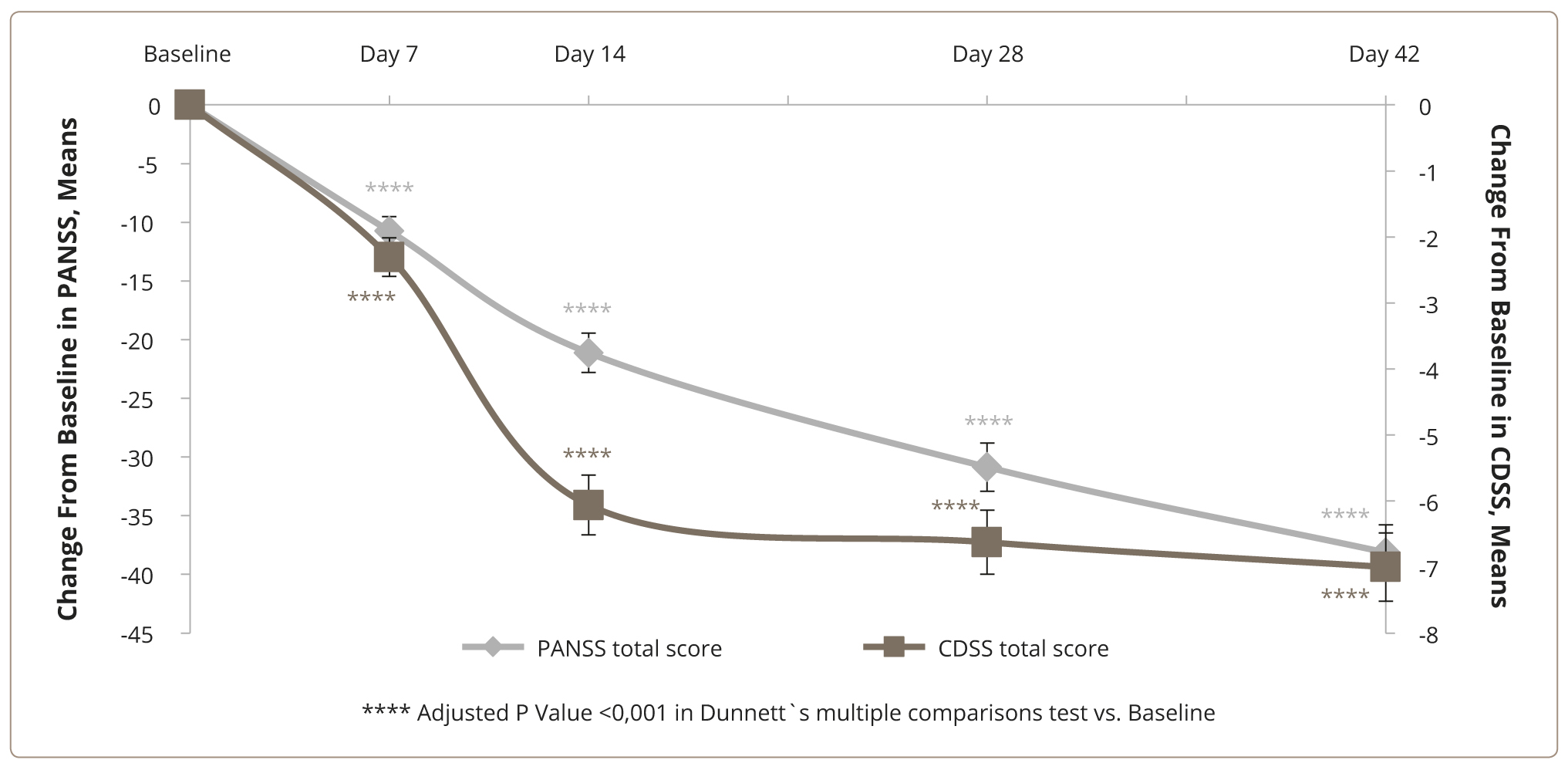
Figure 1. Changes in the total PANSS and CDSS scores.
Table 2. Primary (CDSS total score) and secondary (PANSS positive subscale, negative subscale, general psychopathology subscale, PANSS total score) outcome variables for Repeated Measures ANOVA Results
|
Scale / subscale |
df |
Sum of Squares |
Mean Square |
F |
F (DFn, DFd) |
p |
ηp2 |
|
CDSS total score |
4 |
6324.73 |
1581.18 |
154.36 |
F (1,463, 244,3)=156,7 |
<0.001 |
0.48 |
|
PANSS, positive subscale |
4 |
8672.64 |
2168.16 |
200.88 |
F (1,491, 249,0)=195,5 |
<0.001 |
0.55 |
|
PANSS, negative subscale |
4 |
6728.98 |
1682.25 |
185.99 |
F (1,582, 264,2)=171,9 |
<0.001 |
0.53 |
|
PANSS, general psychopathology subscale |
4 |
37098.85 |
9274.71 |
107.56 |
F (1,593, 266,0)=103,7 |
<0.001 |
0.39 |
|
PANSS total score |
4 |
150164.85 |
37541.21 |
242.39 |
F (1,455, 243,0)=218,6 |
<0.001 |
0.59 |
Table 3. Primary (CDSS total score) and secondary (PANSS positive subscale, negative subscale, general psychopathology subscale, PANSS total score) outcome variables means and mean changes from the background (repeated-measures ANOVA, LOCF)
|
Variable |
Day |
Mean |
S.D. |
CI 95% of the mean |
Mean change |
CI 95% of the mean change |
t |
df |
Dunnett’s p |
|
CDSS total score |
1 |
16.81 |
7.19 |
15.71–17.91 |
|||||
|
7 |
14.51 |
6.95 |
13.45–15.57 |
2.304 |
1.58–3.02 |
7.883 |
167 |
<0.001 |
|
|
14 |
10.75 |
6.46 |
9.76–11.74 |
6.060 |
4.95–7.17 |
13.42 |
167 |
<0.001 |
|
|
28 |
10.19 |
6.49 |
9.19–11.18 |
6.625 |
5.43–7.82 |
13.62 |
167 |
<0.001 |
|
|
42 |
9.81 |
6.65 |
8.79–10.83 |
7.000 |
5.72–8.28 |
13.49 |
167 |
<0.001 |
|
|
PANSS Positive Subscale score |
1 |
22.11 |
5.20 |
21.31–22.90 |
|||||
|
7 |
19.69 |
5.25 |
18.89–20.49 |
2.42 |
1.76–3.08 |
9.03 |
167 |
<0.001 |
|
|
14 |
16.96 |
5.58 |
16.11–17.82 |
5.14 |
4.12–6.16 |
12.45 |
167 |
<0.001 |
|
|
28 |
14.76 |
5.92 |
13.85–15.66 |
7.35 |
6.11–8.60 |
14.57 |
167 |
<0.001 |
|
|
42 |
13.08 |
6.34 |
12.12–14.05 |
9.02 |
7.61–10.44 |
15.74 |
167 |
<0.001 |
|
|
PANSS Negative Subscale score |
1 |
26.65 |
5.60 |
25.79–27.50 |
|||||
|
7 |
24.54 |
5.19 |
23.75–25.34 |
2.11 |
1.40–2.82 |
7.34 |
167 |
<0.001 |
|
|
14 |
22.33 |
5.08 |
21.55–23.10 |
4.32 |
3.41–5.24 |
11.66 |
167 |
<0.001 |
|
|
28 |
20.09 |
5.45 |
19.26–20.92 |
6.56 |
5.40–7.72 |
13.90 |
167 |
<0.001 |
|
|
42 |
18.67 |
6.02 |
17.75–19.59 |
7.98 |
6.62–9.33 |
14.54 |
167 |
<0.001 |
|
|
1 |
55.60 |
12.72 |
53.65–57.54 |
||||||
|
7 |
49.42 |
10.18 |
47.87–50.98 |
0.71 |
4.41–7.93 |
8.65 |
167 |
<0.001 |
|
|
14 |
43.98 |
9.63 |
42.51–45.45 |
0.96 |
9.25–14.00 |
12.11 |
167 |
<0.001 |
|
|
28 |
38.71 |
10.54 |
37.10–40.32 |
1.16 |
14.02–19.76 |
14.51 |
167 |
<0.001 |
|
|
PANSS General psychopathology Subscale score |
42 |
37.24 |
16.01 |
34.79–39.68 |
1.77 |
14.00–22.71 |
10.40 |
167 |
<0.001 |
|
PANSS total score |
1 |
104.35 |
20.12 |
101.28–107.42 |
|||||
|
7 |
93.61 |
17.55 |
90.93–96.30 |
10.74 |
7.71–13.77 |
8.74 |
167 |
<0.001 |
|
|
14 |
83.23 |
17.90 |
80.50–85.97 |
21.12 |
17.02–25.22 |
12.71 |
167 |
<0.001 |
|
|
28 |
73.49 |
20.17 |
70.41–76.57 |
30.86 |
25.83–35.90 |
15.10 |
167 |
<0.001 |
|
|
42 |
66.21 |
23.12 |
62.68–69.75 |
38.14 |
32.32–43.95 |
16.16 |
167 |
<0.001 |
We assessed the rate of symptom reduction according to the PANSS and CDSS and found a significant difference in favor of depressive symptom reduction by Week 2.
Correlation between the mean dose of lurasidone and the mental status
Some 13 (8%) patients took the drug at a dose of 40 to 80 mg, 87 patients (53.7%) — over 80 mg and up to 120 mg; and 62 (38.3 %) — over 120 mg and up to 160 mg. Repeated measures ANOVA showed no significant interaction effect between the lurasidone dose and treatment duration on the total CDSS score (F (8,660)=1.383, p=0.200).
Assessment of the total PANSS score revealed a statistical interaction between the average lurasidone dose and the treatment duration (F(8, 660)=5.479, p <0.001, ηp2=0.06). Figure 2 shows the changes and mean differences in the PANSS total score compared to Visit 1, depending on the dosage. A pairwise comparison of the changes in baseline values at Visit 5 revealed significant differences between doses of over 80 mg and up to 120 mg per day, doses from 40 to 80 mg per day, and over 120 to 160 mg per day (mean difference [95% CI]: 23.85 [11.12, 36.58], t=4.484, p <0.001 and 10.92 [2.56, 19.27], t=3.127, p=0.006, respectively). Doses over 80 mg and up to 120 mg per day were found to be superior.
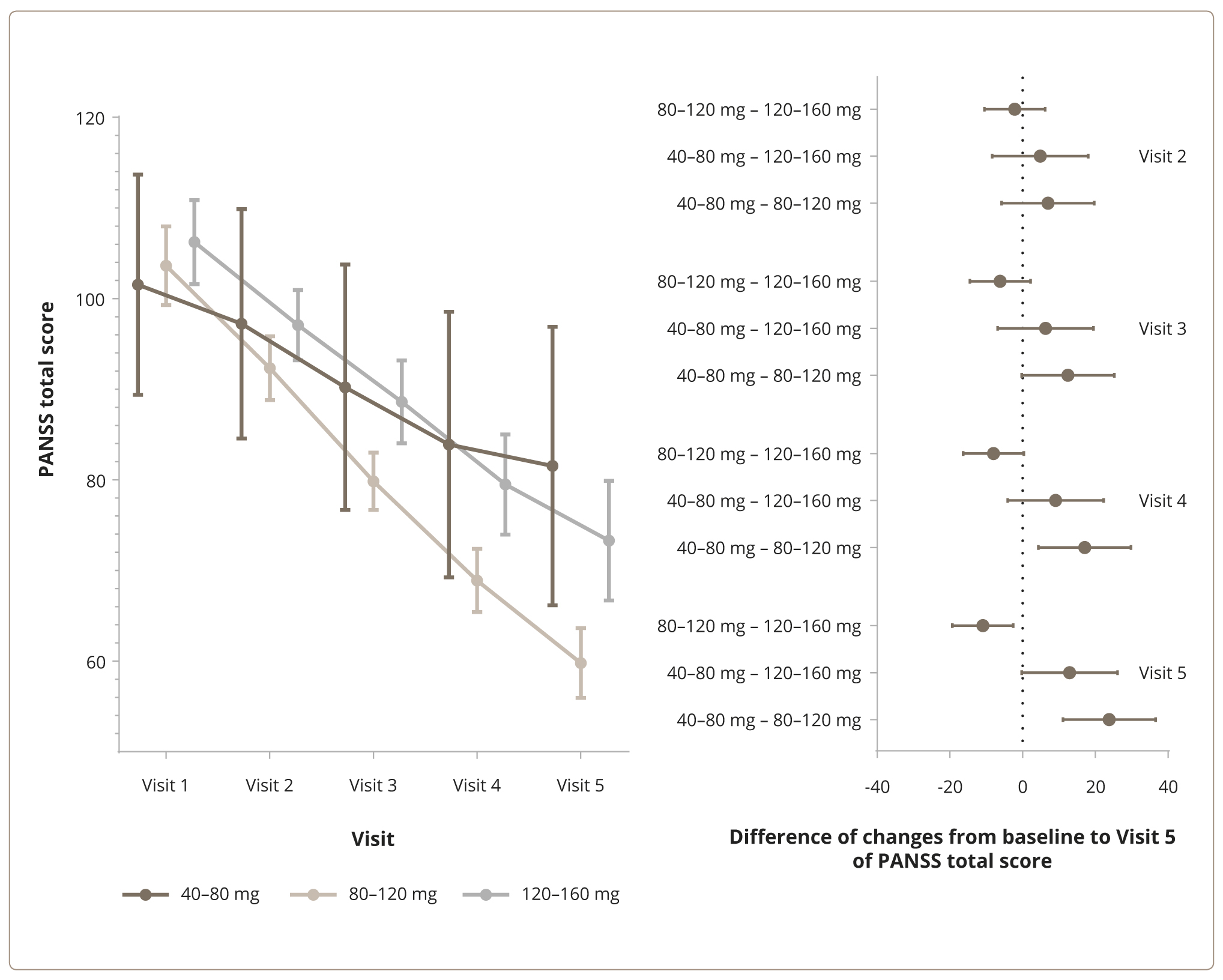
Figure 2. Changes in the total score (left) and mean differences compared to Visit 1 (right) according to the PANSS and the average daily doses of lurasidone: from 40 mg to 80 mg, over 80 and up to 120 mg, and over 120 mg and up to 160 mg.
Twenty-seven patients completed the study ahead of schedule. Among them, five patients (38.5% of all the patients taking lurasidone in this dose range) took the drug at a daily dose of 40–80 mg, eight (9.2%) patients at 80–120 mg, and 14 (22.6%) patients at 120–160 mg. The median [95% CI] duration of participation was 31.79 [21.328–42.244], 60.48 [57.248–63.710], and 52.26 [46.613–57.903] among patients taking lurasidone at a dose of 40–80 mg per day, 80–120 mg per day, and 120–160 mg per day, respectively. Figure 3 shows the results of a Kaplan-Meier survival analysis among patients treated with lurasidone at daily doses of 40–80 mg, 80–120 mg, and 120–160 mg, respectively. A dose range of 80–120 mg was associated with a statistically longer use of lurasidone compared to the dose ranges (i.e., 40–80 mg) (Restricted Mean Survival Time (RMST) Difference [95% CI]: 20 [4–37] days, z=1.488, p=0.01) and 120–160 mg (mean [95% CI] difference: 8 [1–14] days, z=2.31, p=0.02).
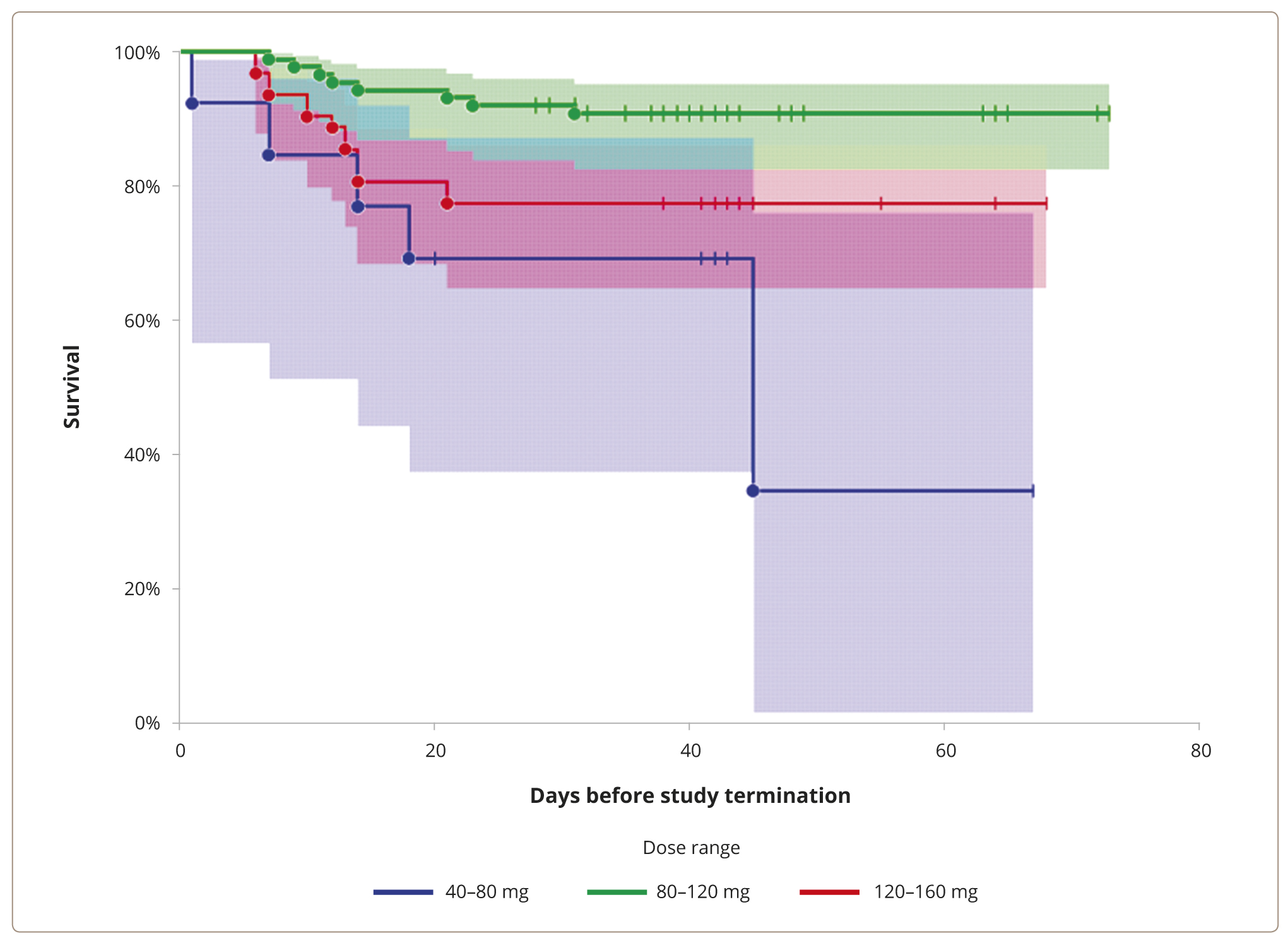
Figure 3. The Kaplan-Meier survival analysis of dosage: from 40 mg to 80 mg, over 80 mg and up to 120 mg, and over 120 mg and up to 160 mg.
Tolerability analysis
Total lurasidone exposure was 657,120 mg, and the total treatment duration was 6,207 person-days.
The study recorded 143 adverse events (AEs) among 85 patients. A complete list of the AEs is given in the Appendix. The most common (in >5% of patients) AEs were: akathisia, in 22 patients (13%); nausea, in 19 patients (11%); tremor, in 14 patients (8%); drowsiness, in 12 patients (7%); headache, in 11 patients (7%); and sleep disruption, in 8 patients (5%). Among 143 AEs, 71 (49.7%) were mild; 60 (42.0%), moderate; and 12 (8.4%), severe. Ten cases of AEs led to premature study termination: two cases of acute dystonia, two cases of tremor, two cases of night sleep disturbance, increased drowsiness, akathisia, pneumonia, and seizures. Overall, the majority of AEs (131 (91.6%) cases) occurred within the first week of therapy, with 22 (17.8%) cases lasting more than one week.
We found a correlation between the mean number of AEs and the average daily dose (F=3.41, p=0.035, one-way ANOVA). The mean daily dose of 40–80 mg corresponded to 0.37 AEs, 80–120 mg per day corresponded to 0.8 AEs, and 120–160 mg per day corresponded to 1.06 AEs. A pairwise post-hoc analysis uncovered statistical differences in mean AE rates between the 40–80 mg per day and 120–160 mg per day dose ranges (mean difference 0.7 [0.03–1.37], t=2.54, p=0.012). A table of the AE incidence and average daily dose is given in the Appendix.
DISCUSSION
This short-duration prospective observational study of the effectiveness of lurasidone in a dose ranging from 40 mg to 160 mg per day has established statistically and clinically significant improvement in both psychotic and depressive symptoms for patients with acute exacerbation of schizophrenia and depressive symptoms. Significant reductions in the PANSS and CDSS scores were noted at all lurasidone dosages (from 40 mg to 160 mg daily) starting with Week 1 of the follow-up period. There is extensive data on lurasidone effectiveness in a situation of acute exacerbations and long-term maintenance of schizophrenia [25, 36, 38, 41], as well as in the treatment of depression [35, 40, 44]. The antipsychotic activity of the drug established in this study was comparable to the results achieved in short-term randomized controlled trials (RCTs) [36, 38]. This study demonstrated the reality of a statistical reduction in the severity of psychotic and depressive symptoms for patients treated with lurasidone at doses of 40 mg to 160 mg per day. However, lurasidone at a daily dose of 120 mg reduced the total PANSS score considerably more than at doses of 40 mg to 80 mg, and over 120 mg (mean difference 23.85 [11.12, 36.58], t=4.484, p <0.001 and 10.92 [2.56, 19.27], t=3.127, p=0.006, respectively). In our opinion, the lower effectiveness of lurasidone at a dose of 160 mg in this study has to do with potential resistance to the treatment among those who were advanced to that dose after insufficient improvement at a 80–120 mg dose level. Also, it is possible that a longer observation period of treatment at 160 mg could yield different results [48]. However, a statistical decrease in the total PANSS and CDSS scores was observed at the end of Week 1 for a dose of lurasidone of 80 mg per day. This suggests that treatment for exacerbations of schizophrenia, associated with depression, should be started at 80 mg per day; the dose should then be gradually increased based on effectiveness, safety, and tolerability. The largest reduction in the total PANSS and CDSS scores with lurasidone at 120 mg per day was associated with the best survival rate and the longest median time from treatment or follow-up initiation to discontinuation.
Our results confirm that lurasidone carries a low risk of weight gain, metabolic disorders, movement or serotonergic disorders. The most commonly reported side effects (e.g., nausea, akathisia, tremor, and drowsiness) in our study were consistent with the known drug safety profile. For example, the frequency of akathisia was 13%; nausea — 11%; tremor — 8%; and drowsiness and headache — 7%. All adverse events were mild or moderate. At the same time, lurasidone at a dose of 120 mg per day was not associated with a higher frequency or severity of adverse events compared to a dose of 80 mg per day. The lurasidone safety profile is consistent with previously published RCT data [38, 41, 49].
Study limitations
To date, there exist a variety of views on the combination of depression and schizophrenia and their clinical signs. This leads to possible clinical and psychopathological diversity amongst study results. It may be related to the individual variability in the effect of lurasidone. This study was not blinded and did not include a control group. We suspect that the improvement in depression was the result of the positive effect deriving from participation in the observational study itself or the expectation of a positive result by the physician, rather than as a direct effect of the drug. At the same time, patients continued to receive their standard psychiatric care and management without any additional research interventions. Limitations also include the relatively short duration of the follow-up period. Then, further studies on the long-term effectiveness of lurasidone in patients with schizophrenia and depressive symptoms are needed.
Implementation into practice
We report on the results of the first Russian multicenter observational study of the effectiveness of lurasidone in patients with acute episodes of schizophrenia and associated symptoms of depression. This study showed that six weeks of lurasidone therapy at doses of 40 to 160 mg per day provided a significant improvement in the CDSS (primary effectiveness endpoint) and PANSS (key secondary effectiveness endpoint) total scores and other secondary effectiveness endpoints (positive and negative symptom scores). We documented side effects of lurasidone such as nausea, akathisia, drowsiness, and minimal effect on body weight and metabolic parameters. These side effects are consistent with the safety profile reported in randomized controlled trials. The study confirmed that lurasidone is effective and well-tolerated in the treatment of acute episodes of schizophrenia and associated symptoms of depression.
CONCLUSION
A six-week prospective observational study of the real-world clinical effectiveness of lurasidone in doses ranging from 40 mg to 160 mg per day established statistically and clinically significant improvements in both psychotic and depressive symptoms in patients with acute exacerbation of schizophrenia and associated symptoms of depression. Lurasidone proved overall safe and well-tolerated, with little effect on weight, metabolic, or endocrine parameters, and even on the neurological status of the patients.