INTRODUCTION
Thailand is an upper middle-income country (UMIC) located in the center of mainland Southeast Asia with a population of 66.17 million as of 2021[1–6]. Like other UMICs, mental health problems are significant and the mental health gap in service accessibility remains an issue [7]. This gap proved wider during the COVID-19 pandemic, in which a strengthened community mental health service could have been key in remedying the situation.
Looking into the community mental health system of Thailand with the help of the World Health Organization Assessment Instrument for Mental Health Systems (WHO-AIMS) Version 2.2, 2005, could help provide a comprehensive overview of the system and a plausible solution as to how to reduce the gaps in mental health provision in the country. WHO-AIMS consists of a policy and legislative framework, mental health service, mental health in primary care, human resources, public education and links with other sectors, as well as monitoring and research [8].
The aim of this article is to review the development of community mental health in Thailand. This article was divided into five main sections: the mental health service system in Thailand, the community mental health system, human resources in the community mental health system, mental health financing, public education, and links to other sectors. The details of each section are illustrated below.
MENTAL HEALTH SERVICE SYSTEM IN THAILAND
Prevalence of mental disorders and mental health problems
According to the 2013 Thailand National Mental Health Survey, the lifetime rate of prevalence of mental disorders stood at 7.4% (3.9 million people) of the population. The lifetime rate of prevalence of major psychiatric diseases was 1.1% for psychosis [9], 0.2% for bipolar disorder, 1.6% for major depressive disorder, and 3.1% for anxiety disorders [7]. For any substance use disorder, lifetime prevalence was 26.5% of the population, while for alcohol use disorders, drug use disorders, and nicotine dependence stood at 18.0%, 4.1% and 14.9%, respectively [7]. In children, the prevalence of autism spectrum disorder was 0.47% in children (0–5 years) and 0.8% in school-age children (5–12 years), respectively [10]. While the prevalence of Attention Deficit Hyperactivity Disorder (ADHD) among Thai children was 8.1%, the frequency of depression among Thai adolescents stood at 17.5% [11, 12].
Not only mental disorders, but follow-up mental health problems were also placed at the center of concern in the country’s community mental health system. The prevalence of suicides in 2020 was at least 7.37 per 100,000 population [13]. In the same year, the Department of Mental Health developed a passive surveillance system for mental health problems focusing on a high level of stress, reported symptoms of depression, and risk of suicide, including burnout, called “Mental Health Check-In.” This instrument served as a digital platform self-assessment tool online to detect the risk of the aforementioned mental health problems among Thais. From January 1, 2020, to April 30, 2022, there were 3,186,935 cases who assessed their mental health status through the “Mental Health Check-In” system during the COVID-19 pandemic. The results showed that the prevalence rates of a self-reported high level of stress, risk of depression, risk of suicide, and burnout were 7.48%, 8.83%, 4.87%, and 4.19%, respectively [14].
Organization of mental health care
Mental health services in Thailand were incepted in 1889, when the first psychiatric hospital began to operate, followed by many regional hospitals throughout the country [1]. In 1977–1978, the project Monitoring Mental Health Needs (in cooperation with the World Health Organization) demonstrated that community mental health services were required. Since then, mental health services have extended from the psychiatric hospital to the public health care system. Mental health care has been integrated into primary care since 1982, resulting in a major change to begin focusing on mental health at the community level [1, 15].
Currently, there are 13 areas in the country where health services are available, including Bangkok [16]. The 13 regional mental health centers under the Department of Mental Health, Ministry of Public Health, play an important role in community mental health provision in the implementation of mental health policy by coordinating, facilitating, and supporting the local community mental health network that includes provincial general hospitals, community hospitals, and primary care units in each province to integrate mental health into their activities [1, 16–17]. Psychiatric hospitals also play an important role in supporting the community care provided by the local community / general hospital, and training health personnel working in mental health care [1, 16]. The role of the Thai Ministry of Public Health (regulator, service provider, integrator) is shown in Figure 1. However, mental health care services are available in university hospitals and military hospitals under other ministries, such as the Ministry of Higher Education, Science, Research and Innovation, as well as the Ministry of Defense.
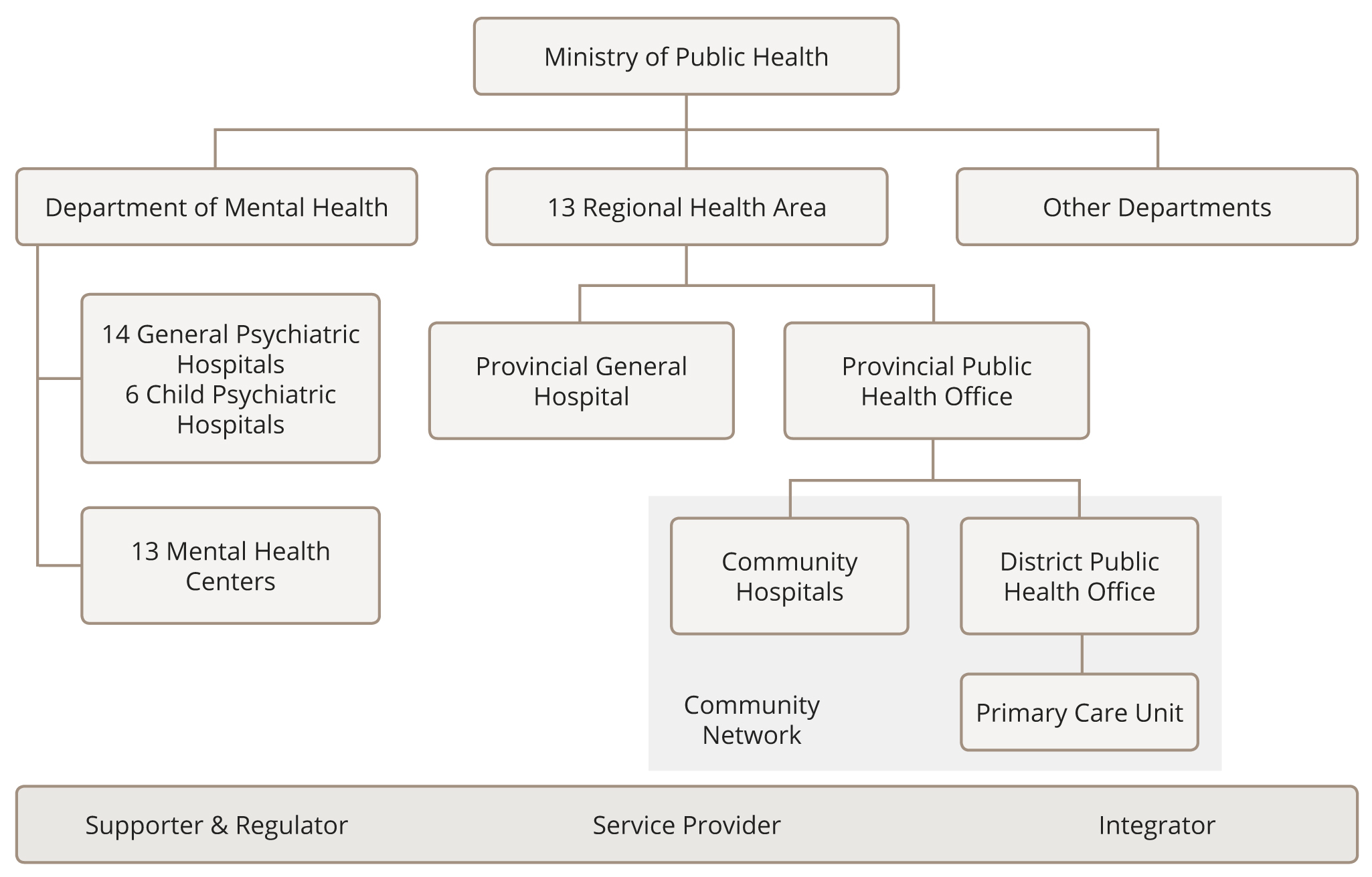
Figure 1. Functions of the Thai Ministry of Public Health (regulator, service provider, integrator) [17, 19].
Thailand has 20 mental / psychiatric hospitals, distributed throughout all the regions of the country, providing specialized psychiatric care as centers of excellence with continuous quality improvement of service. Moreover, there are 20 outpatient mental health facilities attached to mental hospitals, six of them specifically for children and adolescents [18]. There are medical school hospitals and military hospitals that also provide specialized outpatient mental health services. Details of both hospital and outpatient facilities will be described later.
Mental Health Policy and Legislative Framework
Mental health policy was initially formulated in 1995. The policy aims to promote mental health, prevent mental health problems, and provide access to quality mental health care through treatment and rehabilitation that are integrated into public health care. Strategies focus on 1) academic and technical development through research and knowledge management; 2) distribution and empowerment of integrated mental health care in the public health system and mental health network; 3) development of mental health personnel; 4) reforming the organizational management system 5); and development of community mental health services and a mental health component in primary health care, including quality improvement [1, 15]. Mental health services are organized in terms of catchment/service areas [15].
Mental health legislation has been in place since 2008. The Department of Mental Health, as an expression of the Ministry of Public Health, is responsible for the implementation and administration of the Mental Health Act (2008), and it issues regulations and notifications for the execution of the Act. The National Mental Health Board is the mechanism used to formulate policy and measures related to the protection of the rights of people with mental disorders and ensure their access to mental health services and social inclusion. The board also has the duty to inspect and monitor the standards in mental health practice [16]. Its charge thus includes ensuring access to mental health care, including access to the least restrictive type of care; protecting the rights of consumers of mental health services, the family and other care providers; ensuring competence; monitoring capacity and guardianship issues for people with mental illnesses; voluntary and involuntary treatment; law enforcement and other issues of the judicial system for people with mental illnesses; and devising the mechanisms to oversee involuntary admission and treatment practices and the mechanisms to implement the provision of mental health legislation [15, 20–21].
In 2018, the Mental Health Act Revised Version was signed into law. It authorized the National Mental Health Commission to put in place measures to promote mental health and to work on prevention in both the health and non-health sectors. In the new version, community mental health was highlighted, as it included the strengthening of actions in the field of mental health in non-health sectors [21].
According to the 20-year national mental health plan (2018–2037), approved by the National Mental Health Commission in 2018, the four strategies included in the plan were as follows: 1) promotion of mental health and prevention of mental disorders throughout peoples’ lifespan; 2) strengthening of the mental health service infrastructure; 3) devising social welfare and legislation strategies; and 4) academic and technical development through research and knowledge management. The vision in this mental health plan can be captured in the statement “All Thais have good emotional intelligence, happiness, and a valuable life in society” [22].
Mental health inpatient facilities
All mental / psychiatric hospitals are organizationally integrated with mental health outpatient facilities. Some medical school hospitals and military hospitals, including some hospitals at the regional levels also provide inpatient psychiatric care [15, 17–18].
Most of the psychiatric beds in the country are provided by mental / psychiatric hospitals, with 6.26 mental hospital beds per 100,000 population and have 126.27 annual admissions per 100,000 population [18]. However, there are four hospital facilities available specifically for children and adolescents, which provide 2.98 hospital beds for children and adolescents per 100,000 population and have 106.65 annual admissions per 100,000 population [18]. In the last three years (2019–2021), the number of beds in mental hospitals has remained the same; however, the occupancy rate has decreased from 87.06% in 2019 to 75.05% in 2020 and 64.09% in 2021 due to the pandemic [19]. It has been established that 75.25% of the total number of patients have had a stay at a mental hospital of less than 1 year [18]. During 2019–2021, the average number of days spent in mental hospitals was 26, 25, and 23, respectively. However, data on diagnoses were not available [19].
In addition, there are inpatient psychiatric units in 18 general hospitals. However, data on the number of beds in general hospital psychiatric units and annual admissions per 100,000 population were unavailable to us [18]. There are 116 community residential facilities with 1.67 community residential beds per 100,000 population [18]. In terms of treatment, all community inpatient units boast at least one psychotropic drug of each therapeutic class available in the facility throughout the year [15]. Although a growing number of government hospitals have expanded to provide mental health services in response to a growing need, such hospitals are still struggling to offer adequate inpatient psychiatric beds [16]. After discharge from the inpatient psychiatric unit, most patients will be followed up in the same hospital until they are stable enough to be referred for follow-up to their family physicians or general practitioners in their community hospitals.
Mental health outpatient facilities
As previously described, there are outpatient facilities at mental hospitals, medical school hospitals, and military hospitals in Thailand. Moreover, 720 community / nonhospital mental health outpatient facilities and 378 other outpatient facilities (for example, mental health daycare or treatment facility) are also available [18]. However, no facility has mobile mental health clinic teams. As is the case with inpatient facilities, all outpatient facilities also have at least one psychotropic drug of each therapeutic class available throughout the year [15]. The number of visits made by service users in 2020 to outpatient mental health facilities attached to a hospital and to an outpatient facility specifically catered to children and adolescents amounted to 12,838.23 and 1,113.69 visits per 100,000 population, respectively [18].
THE COMMUNITY MENTAL HEALTH SYSTEM
Community mental health provision has been a reality in Thailand since 1964, a history of more than half a century. It was started with the dispatching of mental health mobile teams to provide services in remote areas where people had no access to such services. However, coverage was limited due to a lack of resources. In 1976, in collaboration with the WHO, a project called “Monitoring Mental Health Needs” was started to provide mental health services in communities. Thus, community mental health services began to expand from psychiatric hospitals to the public health care system [1]. Today, community mental health has reached the point where it covers the needs of the population throughout their lifetime in all aspects: promotion, prevention, treatment, and rehabilitation [21].
Community mental health facilities
Community mental health care has been integrated into the public health care system under the Ministry of Public Health’s infrastructure from the village level to the regional level, as demonstrated in Figure 1. Within the public health care sector, local health personnel work in the community with the support of the Department of Mental Health, the multidisciplinary mental health team in regional hospitals, the mental health team in general/ community hospitals, local health personnel in primary health care centers, and village health volunteers in the local community [1].
Due to the shortage of mental health personnel, strengthening the capacity of local people to provide quality and sustainable care in collaboration with stakeholders in the community mental health network is the most important goal [1, 16]. Additionally, community mental health has been extended to networks outside the health care system, including schools, temples, and community leaders. Cooperation with community leaders is an important factor in the success of what is done at the level of community mental health care [1]. As a result, community hospitals throughout the country have continued to strengthen their ability to provide primary and community-based mental health care, while regional and provincial hospitals have developed psychiatric clinics, inpatient units, and psychiatric supervision.
After the 2012 health care reform, the role of the Department of Mental Health expanded to include the development of mental health policy and regulation of the mental health services sector at the provincial and district levels [16].
However, compared to the WHO “pyramid” model, there are no stand-alone community mental health centers available in Thailand because our country has already integrated its mental health infrastructure up to the community level (Figure 2) [1].
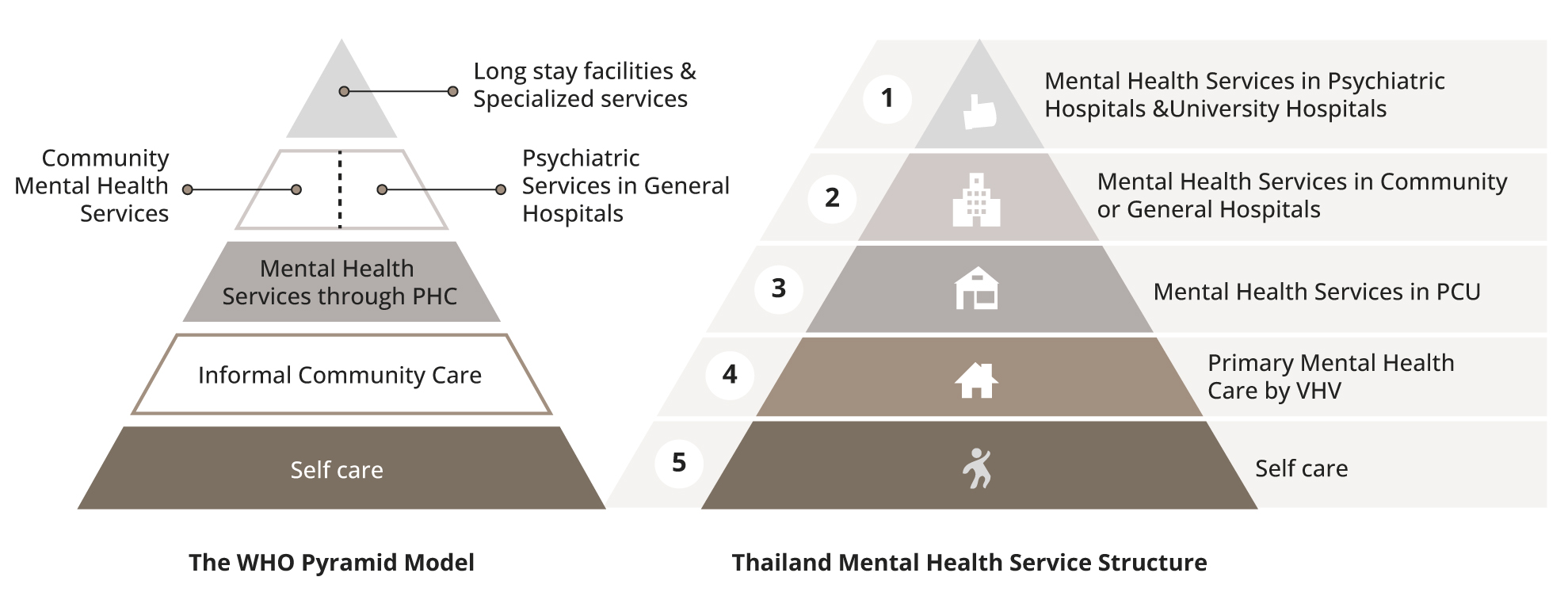
Figure 2. Structure of mental health services in Thailand compared to the WHO pyramid model [adapted from reference number 1]. Note: PHC=Primary Health Care; PCU=Primary care unit; VHV=Village Health Volunteers.
The stages of health services delivery are sorted into four levels as follows [16]:
1) Self-care at the family level: includes the empowerment of people’s ability to provide self-care and make decisions about their own health.
2) Primary health care level: includes activities organized by the community to provide services related to health promotion and prevention.
- a) Primary mental health care at the village level: This level encourages participation of the community in mental health activities by village health volunteers, the central community mental health care personnel [1].
- b) Subdistrict level (Health center, community health facilities): This level provides primary medical services, including mental health screening and monitoring to ensure continuity in psychiatric care by the health personnel of the primary care units and health centers [1].
- c) District level (Community Hospital): This level provides outpatient services for common psychiatric disorders, continuity of care for chronic patients, and mental health care for general hospital patients by primary physicians [1]. These physicians are allowed to prescribe psychotropic drugs. Nonetheless, human resource capacity, especially the development of psychiatric nursing at the district level, is emphasized due to the lack of specialized mental health personnel and budget shortfall [1]. Mental health nurses can prescribe low-risk psychotropic drugs countersigned by a family physician or general physician [15].
3) Secondary health care level (General hospitals and some regional hospitals): Secondary health care is managed by specialized medical and health personnel. General hospitals at the provincial level provide outpatient services for common psychiatric disorders, continuity of care for chronic patients, and mental health care for general hospital patients [1].
4) Tertiary health care (University hospitals, psychiatric hospitals or institutes, and some regional hospitals): This level provides specialized, comprehensive psychiatric care [1].
Mental health care at each level includes not only psychiatric care and rehabilitation, but also preventive care and promotion of mental health. In the deinstitutionalization policy, the strengthening of community mental health services provision is much more emphasized than is the downsizing of psychiatric hospitals [1]. According to the Mental Health Atlas, the number of community-based mental health facilities per 100,000 population stood at1.69/100,000 in 2020 [18].
All hospitals / institutes must improve their quality of service according to the standards established by the Institute of Hospital Quality Improvement and Accreditation, which is called Hospital Accreditation (HA). Mental health is one of the domains evaluated by HA [1].
Community mental health in primary care
Based on the WHO’s Health for All by the Year 2000 policy of 1978, Thailand added “mental health” to the essential components of its “basic primary health care’,” which led to the integration of mental health services at the community level [1].
In 1997, the Mental Health Center was established according to regional health zones to facilitate and support the community mental health network, especially in promotion and prevention [1]. After the reform of the Department of Mental Health in 2012, several bureaus were established to effectively administer the mental health system [17]. All of these bureaus are involved at different levels of mental health care provision in primary health care units as follows.
Promoting Self-Care at the community level: The aim is to promote mental wellbeing in the general population [1]. In preschoolers, parents and families are provided with means for early-childhood-development monitoring and helped to promote their children’s development at home [19]. Recently, “Mental Health Check-in” has been promoted for self-monitoring and self-care in the sphere of mental health [19]. Volunteers and healthcare personnel also collaborate to provide mental health and social support to patients with psychiatric disorders and their caregivers, both in the community and in the hospital, as well as the implementation of psychosocial support and prevention programs [16].
Mental health care in the primary care unit: Detection of mental health problems by village health volunteers plays a critical role in community mental health [1]. Due to the presence of village health volunteers in each community (one per 10 households), the mental health services in primary health care provided by trained village health volunteers and primary care staffs include mental health education; early detection of mental health problems such as psychosis, autism, depression, and suicide; provision of psychological support; and facilitating continued care or community rehabilitation [1]. They also play supporting roles for patients and caregivers in the proper use of psychotropic drugs and encourage patients to continue their medications regularly [16].
Integrating mental health care into the medical care service: The majority of patients in primary care are persons with noncommunicable diseases (NCD): eg, diabetes mellitus, hypertension, dyslipidemia, etc. Medical illnesses and mental disorders are significantly interrelated and both conditions can be found in comorbidity with each other. Therefore, holistic care for these patients needs an element of psychosocial care, especially for difficult cases of NCD. Brief advice, brief intervention, and disease-related behavioral modifications are examples of mental health care that can be provided in NCD clinics [17].
Referral to secondary health care: For complicated mental disorders, referral from the primary to secondary level of the health care system is crucial. Currently, 91.7% of community hospitals and 100% of general hospitals can provide outpatient services for the early management of common psychiatric disorders, continued care of chronic patients; crisis intervention, supervision of primary health care and primary medical care, and integration of mental health care into general medical care [1]. For inpatient services, there are 102 community/ general/ regional hospitals in many provinces in Thailand with at least one psychiatrist to provide inpatient services within the province [23].
Treatment and rehabilitation of mental disorders in the community mental health system
Treatment of and rehabilitation from mental disorders has focused on schizophrenia and depression/depressive disorders.
For schizophrenia: Regular home visits by village health volunteers or primary care staffs were effective in improving drug compliance, as proved in the “F20 project.” The project has expanded to include patients with serious mental illnesses with violence (SMI-V), in which police and the community must collaborate with the community hospital staff to transfer these patients to a hospital safely [24].
For depression/ depressive disorders: High-risk persons after a 2Q/9Q screening test [25–26] have been referred to community hospitals for diagnosis and proper management. Pharmacotherapy and mental health counseling can be provided at the level of a community hospital. For people with complicated conditions, referral to general or mental hospitals can be made as part of the staggered care model [27].
Beyond normal situations, the mental health team at the community hospital is trained to be a “Mental Health Crisis Assessment and Treatment Team” (MCATT) in order to provide mental health care in natural or man-made crises. The MCATT is also a part of the public health emergency response team [19].
Mental health promotion and prevention in community mental health
Mental health promotion and prevention is undertaken according to age groups; that is, maternal and early-childhood, school-aged children and adolescents, adults, and the elderly.
For maternal and early childhood: Detection of depression during pregnancy has been integrated into antenatal care, which is performed at all levels of the health care provision [27]. Since 2015, the Early Childhood Development Monitoring and Promotion Program has been applied at the level of the vaccination clinic in primary care centers and, also, in early childhood centers. By applying the holistic approach in following the development of preschool children with the aim of increasing the awareness of parents about their child’s level of development and literacy and encourage self-intervention in the lives of those children. Currently, approximately 60% of children are at risk of stunt development. They have been identified and recruited into the public health care system [19, 28].
In school-age children and adolescents: There is a link between hospitals and schools called the Health and Educational Regional Operations (HERO) program for schools, which is an intersectoral collaboration between the health and educational sectors. It is a timely and innovative platform for the monitoring, support, and care for vulnerable students. The platform serves as a tool for teachers in screening for mental health problems and for management of uncomplicated behavioral and emotional problems through behavioral modification or counseling, respectively [29]. Children who cannot be helped through school-based care are referred to a community hospital through the digital platform School Health HERO [29]. The community hospital staff who provide consultation on mental health care for such a group of children have been called “HERO consultants”.
For adulthood: Lookout for depression and screening tests using 2Q/9Q questionnaires have been in place for more than a decade [25–26]. A 10-year review of the project showed that the accessibility rate for those suffering from depression has gone from less than 5% to approximately 50% [27]. During the COVID-19 pandemic, the Department of Mental Health has monitored mental health problems using Mental Health Check-In to allow the general population to check their mental health status and improve their knowledge about mental health. For those at risk of the abovementioned mental health problems (a high level of stress, reported symptoms of depression, and risk of suicide, including burnout ) and who request mental health care, mental hospital and community hospital staff would call back to provide counseling. During the pandemic, 89.15% of those who have requested mental health care have received counseling services [30].
Among the elderly: Mental health promotion focusing on happiness and well-being has been blended into the health promotion package, as well as depression screening. An elderly club has been opened in almost all subdistricts, and healthy elderly people can join such a club. However, two-thirds of the elderly who are partially or totally disabled and cannot join such a club, village health volunteers or primary care personnel will visit them at home to provide health and mental health care [19].
Additionally, the National Suicide Prevention Strategic Plan and Campaign was amended in 2020 as a preventive measure and plan to tackle post-COVID mental health consequences and the suicide rate in Thailand. The campaign consists of an evaluation of suicide conditions, interventions, and referral between the multisector network and health sector [19]. In addition, it has been integrated into the National Committee on Mental Health Act to drive policy and campaign nationally.
Monitoring and Research in Community Mental Health
Mental health policy in Thailand has changed to include integration into the general health care system. This makes the delivery of services focused on accessible health care for the Thai population and the coverage of health service facilities, rather than housing all services in psychiatric hospitals as previously. Successful monitoring is the development of outpatient psychiatric units in district and provincial hospitals, inpatient psychiatric units in each provincial hospital, and the development of rehabilitation and recovery services in psychiatric hospitals [19]. The integration of data regarding most psychiatric services in our country manifests itself in a single health data center located at the Ministry of Public Health, which can be used for further research into community mental health [31].
HUMAN RESOURCES IN COMMUNITY MENTAL HEALTH
Mental health professionals
Some professionals work in both inpatient and outpatient settings. There is a disproportionate amount of resources concentrated in the major cities, which starves rural areas of mental health services[15].
Psychiatrists and other medical doctors
Although the number of psychiatrists (general psychiatrists, child and adolescent psychiatrists, and geriatric psychiatrists) is now better distributed than in the past, most psychiatrists still practice and live in the major cities, including Bangkok [23]. However, there are still not enough children and adolescent psychiatrists, including geriatric psychiatrists, while the need for such professionals is increasing [18]. Most psychiatrists work full-time in hospitals or government-funded mental health facilities [16]. Most psychiatrists (69%) work for government general hospitals, and only 29.1% are employed by psychiatric hospitals [16].
To solve the problem of the shortage of psychiatrists and boost mental health promotion and the prevention of mental disorders, the Department of Mental Health has received permission from the Thai Medical Council to train general doctors to become specialists in preventive medicine focusing on community mental health. These medical doctors will provide system-based mental health services in the community. Their role will be to focus more the mental health promotion and the prevention of mental disorders. In 2021, there were 1,262 doctors that qualified as sub-specialists in preventive medicine focusing on community mental health [32].
General physicians who attend short psychiatric workshop courses [1]. Primary health care physicians have limited experience in undergraduate psychiatric education and interaction with mental health services [15]; therefore, short course psychiatric workshops should be required. Up to now, approximately 1,000 community physicians (general practitioners) have attended such psychiatric/ mental health workshops [16].
Psychiatric nurses
Nursing training courses include a master’s degree (2 years) in mental health nursing or an advanced diploma (at least 4 months) in mental health or in child and adolescent mental health nursing [1]. Moreover, an advanced diploma in geriatric mental health nursing has been unveiled recently. According to a survey conducted in 2013, most nurses who work in community mental health settings have been specifically trained in mental health [16].
Psychologists
Their qualification is a 4-year bachelor’s degree, but certification and registration are required if they want to practice clinically [1]. According to the Geographic Information System (GIS) database of the Bureau of Health Strategy of the Ministry of Public Health, as of 2022, there are 729 psychologists working in health facilities, both psychiatric hospitals and provincial and sub provincial hospitals [31, 33–34].
Social workers
Most of them work in psychiatric and provincial hospitals. Social workers who work in provincial hospitals mostly provide general welfare services, while their counterparts who work in psychiatric hospitals provide mental health services, including psychosocial treatment and rehabilitation [1].
Occupational Therapists (OT)
There are a total of 1,067 occupational therapists working in Thailand [35]. Most OTs are involved in the rehabilitation of patients with medical conditions [1]. However, the number of OTs who work with people with mental illness is limited, and most of them work in psychiatric hospitals [19]. Due to the shortage of OTs working in the mental health field, therefore, some of the responsibilities of the rehabilitation services have been shifted to psychiatric nurses and social workers, working in concert to provide service for people with chronic mental illnesses.
MENTAL HEALTH CARE FINANCING
According to the WHO’s Mental Health Atlas 2020, funding for mental health amounts to only 2.3% of total government health expenditures, which is not adequate [18]. However, 81.2% of the aforementioned 2.3% of funding from the government is directed at mental hospitals [18]. The mental health budget allocated for promotion and education is approximately 3% of the total mental health budget [16]. Data on the mental health budget for community mental health is not available [16].
Thailand already has a developed health services sector and insurance plans that can provide health services to all Thai citizens. There are currently three main health care benefit schemes in the country: 1) the Universal Coverage Scheme, which is a tax-based scheme funded by the Ministry of Public Health, for all Thai citizens; 2) a Social Security Scheme, which is mandatory insurance under the Ministry of Labor for all employees; and 3) the Civil Servant Medical Benefit Scheme for government employees and their dependents (parents and up to three children) [16]. In 2021, 99.57% of Thai citizens were covered by the three main government health insurance schemes [36].
These main health benefits schemes include the cost of mental health care, including free access to the psychotropic drugs on the national essential drug lists that cover all mental disorders at all levels of care [1]. The cost of the referral system, outpatient care, and admission care has also been included [1, 16]. Mental health care funding is allocated to local health facilities, which are responsible for providing the services [1].
PUBLIC EDUCATION AND LINKS WITH OTHER SECTORS
The stigma of mental illness has been found to be widely spread in Thailand [16]. To tackle the problem, public education under multi-sectoral collaboration has been undertaken. The Department of Mental Health established a social mental health bureau to improve mental health literacy through public education [17]. Mental health-related news or phenomena in the country are monitored, and education is readily available to the public about mental health problems or disorders, self-care, and the accessibility of services. The result of that public education can be witnessed in the accessibility rate for patients with depressive disorders, which has gone from less than 5% to more than 50% in approximately 10 years [27].
Furthermore, since there is increasing evidence that mental health literacy can reinforce wellbeing, many efforts must be made to increase awareness about mental health. Therefore, policy to enshrine universal prevention in the Thai population based on the age group has been welcome. In community hospitals, mental health promotion, prevention, treatment, and rehabilitation have been integrated into the general health system.
FUTURE ISSUES FACING COMMUNITY MENTAL HEALTH
Despite the increase in the accessibility of mental health services, some challenging issues remain. First, there is the small number of mental health facilities at the community level, which stood at 1.69 per 100,000 people in 2020 [18], especially facilities providing rehabilitation services. It would be important to develop community health services facilities in the future to help people with chronic, serious mental illnesses reclaim their lives and re-integrate their communities. Second, government funding for mental health is only 2.3% of total government health expenditures [18]. Therefore, it is necessary to advocate for a policy that would encourage investment from other stakeholders in order to improve community mental health services that cover all groups of people in Thailand. Lastly, as the number of long-COVID patients continues to increase and the prevalence of psychiatric symptoms in this group such as sleep problems, anxiety, depression stood at 27.4%, 19.1%, and 12.9%, respectively, the state needs to become even more active. Thus, further research is needed to improve the mental health of patients with long COVID-19 living in communities around the country [37].
CONCLUSION
Although there are no stand-alone community mental health services nodes in Thailand similar to the WHO’s “pyramid” model, community mental health care has been integrated into the general public health care system under the Ministry of Public Health, from the village level to the regional level. After the 2012 health care reform, the role of the Department of Mental Health now includes the development of a mental health policy and the regulation of the mental health services sector at the provincial and district levels. Due to the shortage of mental health personnel in the country, village health volunteers and local health personnel have been strengthening the capacity to provide quality and sustainable mental health care, with the support and collaboration of stakeholders in the community mental health network, including the multidisciplinary mental health team in the Department of Mental Health, and community/ general/regional hospitals. Furthermore, mental health care has been expanded into a network outside the health care system, including schools and community leaders. Several main health insurance schemes support the cost of mental health care at all levels of care, together with a referral system within the public sector. Mental health care at each level includes not only psychiatric care and rehabilitation, but also prevention and promotion of mental health to fill the mental health gap and improve access to services, especially during a pandemic. However, investment in mental health from the government remains insufficient. There are at least three challenges in the future regarding community mental health care provision, such as developing community rehabilitation services facilities for people with chronic, serious mental illnesses; increasing funding from other stakeholders; and mental health care for persons with long COVID.