INTRODUCTION
The development of mental disorders is often associated with a change in a person’s attitude towards themselves and a reassessment of their relationships with those closest to them. In literature, identity transformation in psychotic patients is usually discussed in terms of role reorganization and social maladjustment, self-stigmatization, symptomatic (morbid) personality change, cognitive impairment, as well as opportunities for personal growth [1]. It is of note that the psychological effects of demoralization are not unique to those suffering from psychotic disorders, but in over 20% of cases they are a common response to any serious health challenge [2]. The clinical consequences in this case are associated not only with social maladjustment, but also with psychosomatic, anxiety, and depressive disorders [3]. The consequences of stigmatization as a clinical phenomenon related to demoralization are thus likely to become a “second disease” for some health service users. For patients with mental disorders, the internalization of perceived stigma, developing as a response to social stigma, is particularly common and is associated with impaired recovery, decreased energy capacity, lower self-confidence, and self-efficacy [4, 5]. On the other hand, targeted interventions designed to prevent patients from internalizing perceived stigma and negative social attitudes have shown to be effective with respect to their coping strategies and recovery trajectory [6]. However, the relationship between internalized stigma (IS), feelings of social inadequacy, and low quality of life is being debated, and even when taken together, these factors may not be fully predictive of the breadth of self-stigmatized patients’ behavioral repertoire within the therapeutic process [4]. In particular, adherence to treatment is also largely determined by motivation and the level of one’s insight into the illness [7, 8]. Previous studies have shown higher IS to be associated with poorer treatment adherence across all groups of psychiatric patients [9, 10]. At the same time, in one study, a higher self-rated severity of the illness proved to be a predictor of better adherence to medication, despite the detrimental effect of stigma [11]. It appears that both stigmatization and treatment motivation in psychiatric patients are heterogeneous and multi-dimensional factors, and that their interrelationship may be more complex than previously believed.
Our study aim was to determine the phenomenological subtypes (clusters) of psychiatric stigma as they relate to treatment motivation among inpatients with various mental disorders using a computational approach.
Investigation tasks: (1) to explore IS across its subtypes; and (2) to explore typical associations between types of treatment motivation and IS subtypes.
We tested a hypothesis holding that there is a category of psychiatric patients who can withstand stigma by building a specific structure of treatment motivation. The second assumption was that patients with psychotic disorders and different manifestations of stigmatization present different clinical characteristics.
METHODS
Study design
To address our goal, an observational cohort study design was chosen. Cross-sectional psychosocial variables were used to digitally phenotype groups of patients in a data clustering procedure.
Sample
Patients were recruited from an inpatient unit of the V.M. Bekhterev National Medical Research Centre for Psychiatry and Neurology. Patients were included if they were aged between 18 and 65; were undergoing psychopharmacological treatment for an exacerbation of psychotic, affective, or anxiety disorders or a decompensation of personality disorders (a sample of patients with severe mental disorders [4, 7, 12, 13] for whom the expected levels of psychiatric stigma are the highest); and were close to achieving remission and demonstrated the ability to understand and consent to comply with the research procedures. Patients were excluded if they were unable to participate in assessments due to low cognitive performance, or withdrew consent at any stage.
Ethical approval
Participation in the current study was voluntary and was based on the principles of the Helsinki declaration, confirmed by RIB/IEC (No. 72 EK-I-105/18, dated September 25, 2018).
Measurements
Medical records were used to obtain information about the socio-demographic, clinical, and anamnestic parameters of the patients: sex, age, family status, children, education, occupation, duration of illness, and the number of previous hospitalizations.
All patients in the sample underwent an assessment of treatment motivation and that of the level of IS. Treatment motivation was assessed using The Treatment Motivation Assessment Questionnaire (TMAQ) — based on the patient’s motivation for the psychopharmacotherapy scale, developed at the Department of Integrative pharmaco-psychotherapy [8]. The questionnaire includes 20 items. The mathematical algorithm for their evaluation allows one to extract five standardized indicators in Z-Scores. Structurally, the questionnaire represents 4 motivational factors: (1) reliance on one’s own knowledge and skills to cope with the disorder, (2) insight into treatment necessity, (3) insight into the psychological mechanisms of morbid maladjustment, and (4) willingness to actively participate in the treatment process. All items are rated on a five-point Likert scale (from 1 [strongly disagree] to 5 [strongly agree]), where higher scores reflect higher levels of treatment motivation, with the exception of level 1, where the items are reversely coded. The final internal consistency of TMAQ was found to be good (Cronbach’s alpha 0.842). The convergent, concurrent, and discriminatory validity of the questionnaire was confirmed and described in previous publications [14, 15].
Self-stigmatization was measured using the Russian version of the Internalized Stigma of Mental Illness scale (ISMI) [16]. The validation of the Russian translation of ISMI is currently underway, with findings of the preliminary analysis consistent with the five-factor structure described in the original English version (alienation, stereotype endorsement, perceived discrimination, social withdrawal, and stigma resistance). The original ISMI instrument includes 29 items, each rated on a 4-point scale that ranges from 1 (strongly disagree) to 4 (strongly agree). The results of these questionnaires were used to test the primary hypothesis about the relationship between stigma typology and treatment motivation across the entire sample. The response rate for this part of the study with self-administered questionnaires was 100%. The second hypothesis was tested only in patients with psychotic disorders (schizophrenia, organic mood (with manic features) and schizophrenia-like disorders: codes F2, F06.3, and F06.2 according to ICD-10). The current clinical state of patients was evaluated using the most common psychometric instruments, which also have validated Russian versions: The Brief Psychiatric Rating Scale (BPRS) [17], The Scale for the Assessment of Negative Symptoms (SANS) [18], and The Global Assessment of Functioning scale (GAF) [19]. The response rate for scales application was 93.6%.
Statistical analysis
Analysis of such heterogeneous and dimensional research parameters requires specific statistical tools.
The first stage of the study involved an exploratory analysis with a description of the sample, assessment of the normality of the obtained distributions (using Kolmogorov-Smirnov’s z-test with Lilliefors correction for significance), and a description of the measures of central tendency.
The next step involved the application of a cluster analysis of the sample using the k-means method (IBM SPSS Statistics) for subscales of ISMI (previously standardized using Z-Scores), and factors of the TMAQ (have only Z-Scores measurement) in accordance with accepted statistical and methodological practices [20] commonly applied in practice [12, 21].
Next, a comparison of the socio-demographic and clinical characteristics of the patients within the obtained clusters was performed. The core research analysis was conducted using one-way analysis of variance (ANOVA) and Student’s t-test for parametric data, Kruskal–Wallis H-test and Mann–Whitney U-test for non-parametric data, as well as Pearson’s chi-square test or Fisher’s exact test for nominal scales.
Subsequently, for each obtained cluster, a separate assessment of the nature of the data distribution for the included patients was conducted and measures of central tendency were described using methods similar to those mentioned above.
The next step involved a comparison of the means (or mean ranks, depending on the results of the assessment of the distribution normality) for subscales of IS and subscales evaluating the structure and strength of the treatment motivation of patients, similarly using dispersion analyses. For clarity and consistency, all results were presented as mean values (SD). Differences were considered significant at p ≤0.05.
RESULTS
Sample characteristics
The sample included 63 psychiatric inpatients (ICD-10 diagnostic codes: F2, n=41 (65%); F3, n=8 (13%); F4/F6, n=8 (13%); F06, n=6 (9%)). The mean age of patients was 34±13 years, the mean illness duration was 12±11 years, and 67% of patients were female.
Average values of the main characteristics of interest in the whole sample were as follows. The sum Z-Score of TMAQ (the intensity of motivation for treatment) –0.29 (0.88) and TMAQ factors: reliance on one’s own knowledge and skills to cope with the disorder –0.04 (0.98); insight into treatment necessity -0.08 (0.95); insight into the psychological mechanisms of morbid maladjustment –0.01 (0.92); and willingness to actively participate in the treatment process –0.09 (1.0). The sum score of ISMI (the intensity of self-stigmatization) was 2.47 (0.49); ISMI subscales scores: alienation 2.46 (0.75); stereotype endorsement, 2.12 (0.56); perceived discrimination, 0.11 (0.64); social withdrawal, 2.23 (0.71); and stigma resistance, 3.44 (0.63).
Patients' clusters based on ISMI and TMAQ scores
Cluster analysis of the ISMI scores and TMAQ factors identified three clusters of patients. That enabled us to subtype IS depending on the structure of therapeutic motivation into “explicitly self-stigmatized” (Cluster 1), “implicitly self-stigmatized” (Cluster 2), and patients without specific self-stigmatization marks, i.e., with “minimal self-stigma” (Cluster 3). The results of the cluster analysis are described in Figure 1.
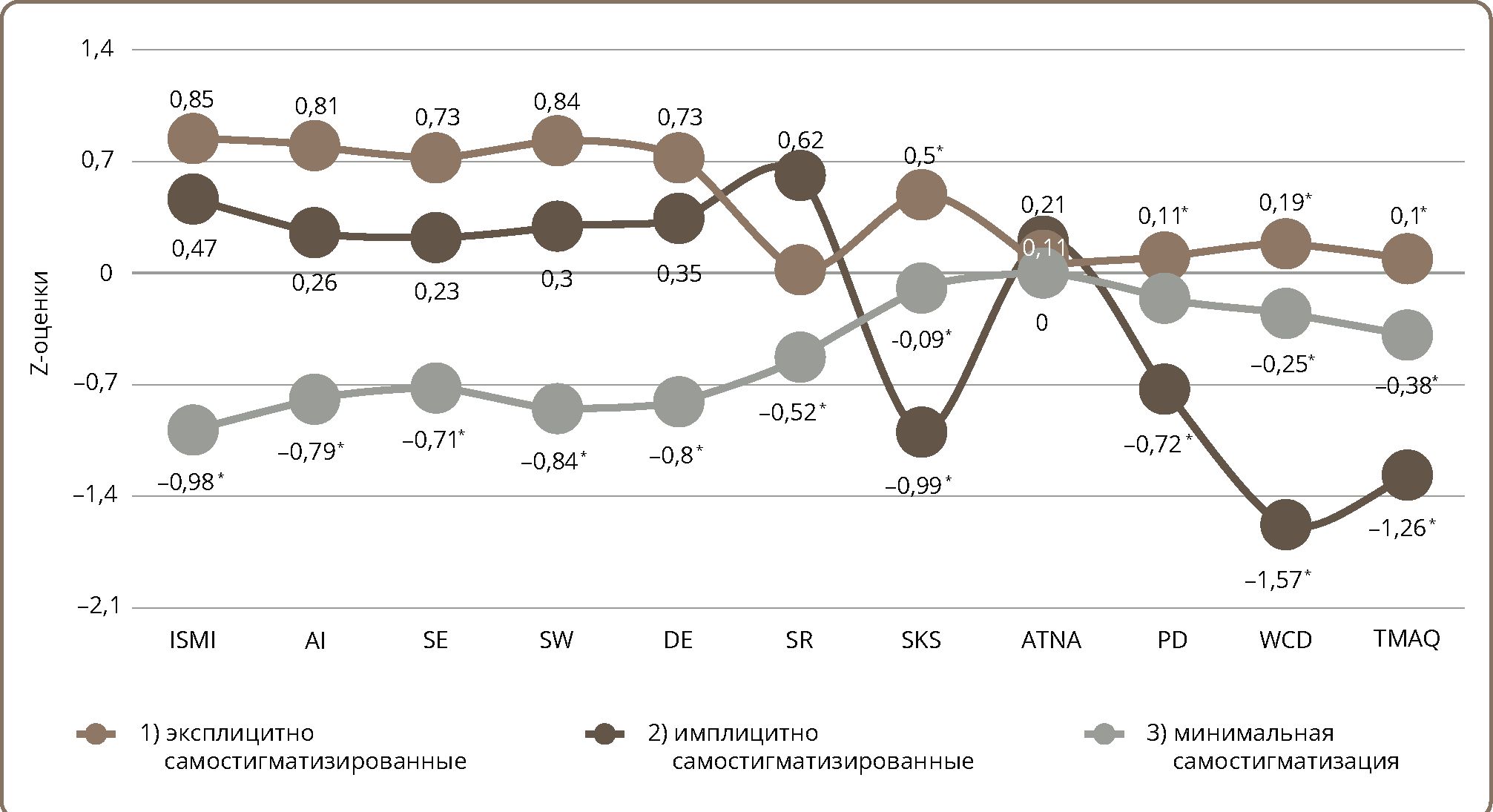
Figure1. Three clusters of IS in connection with treatment motivation in psychiatric inpatients.
Note: * average indicators for a cluster of patients relative to which the indicated numerical values without asterisk differ at p ≤0.05; only values with statistically significant differences are numerically marked. ISMI parameters: ISMI — sum. score, Al — alienation, SE — stereotype endorsement, SW — social withdrawal, DE — discrimination experience, SR — stigma resistance. TMAQ parameters: SKS — reliance on one’s own knowledge and skills to cope with the disorder, ATN — awareness of the treatment necessity, APD — awareness of the psychological mechanism of maladaptation, WCD — willingness to cooperate with doctor, TMAQ — sum. score.
Clinical and demographic characteristics of the patients in clusters
Subjects from the two clusters with self-stigmatization (Cluster 1 and Cluster 2) showed significant differences in all time-associated parameters: age (Cohen’s d=1.1), illness duration (Cohen’s d=2.1), and history of hospitalizations (Cohen’s d=1.3) (Figure 2).
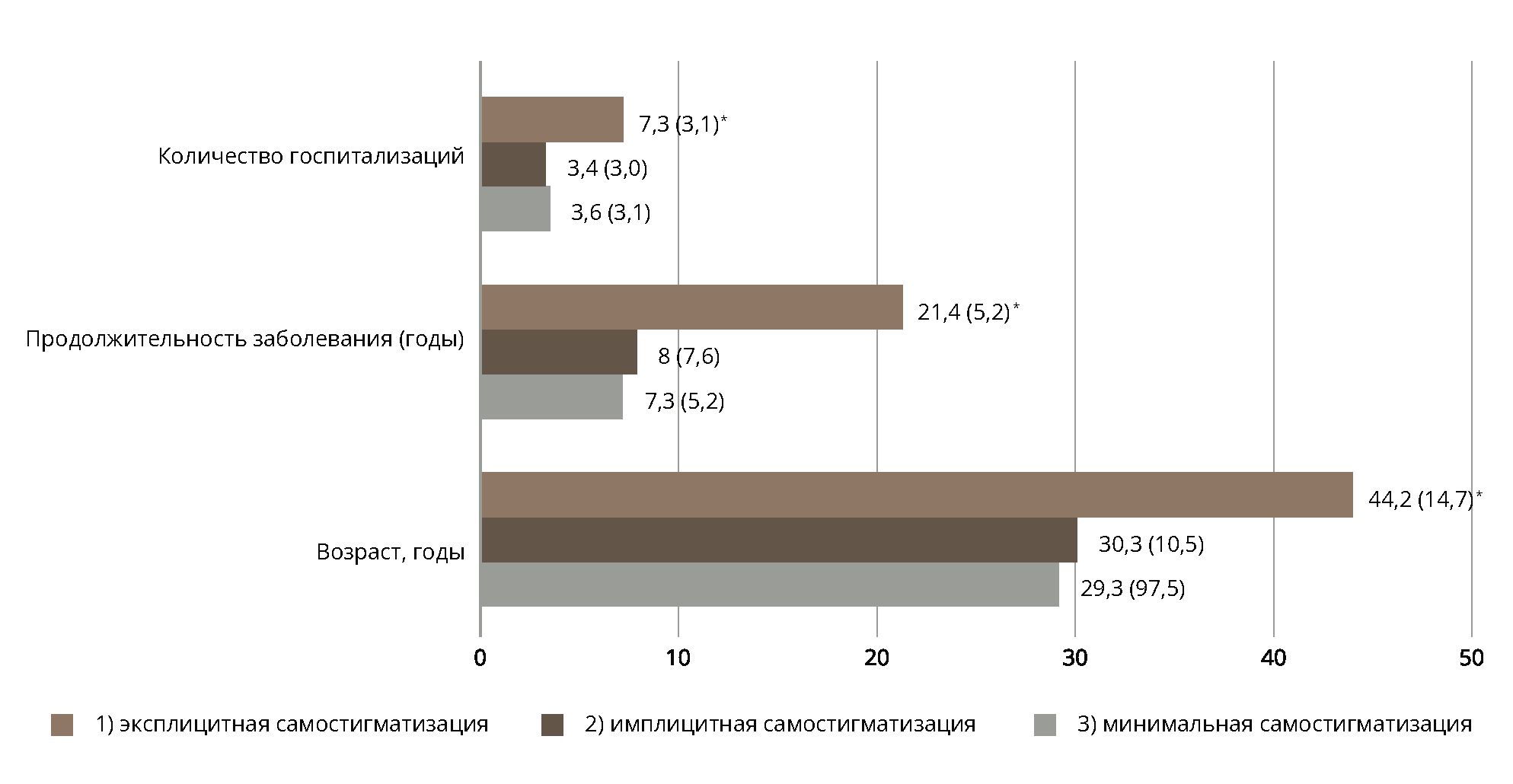
Figure 2. Statistically significant differences between clusters.
Note: * p ≤0.05.
The three resulting clusters of patients showed no differences in main sociodemographic and clinical characteristics, with the exception of the prevalence of negative symptoms and social maladjustment, as well as gender (Table 1 and Table 2).
Table 1. Sociodemographic and clinical characteristics of studied clusters
|
Characteristics |
Prevalence in Cluster, N(%) |
χ2(df) |
|||
|
Cluster 1, n=18 |
Cluster 2, n=20 |
Cluster 3, n=25 |
|||
|
Sex |
Male |
3 (4.8) |
13 (20.6) |
5 (7.9) |
13.3 (2)*** |
|
Female |
15 (23.8) |
7 (11.1) |
20 (31.8) |
||
|
Family |
Married |
6 (9.5) |
6 (9.5) |
9 (14.3) |
0.2 (2) |
|
Single |
12 (19.1) |
14 (22.2) |
16 (25.4) |
||
|
Children |
Yes |
7 (11.1) |
4 (6.4) |
11 (17.5) |
3.0 (2) |
|
No |
11 (17.5) |
16 (25.4) |
14 (22.2) |
||
|
Education |
Primary |
4 (6.4) |
10 (15.8) |
5 (7.9) |
6.0 (4) |
|
Secondary |
5 (7.9) |
3 (4.8) |
5 (7.9) |
||
|
High |
9 (14.3) |
7 (11.1) |
15 (22.7) |
||
|
Occupation |
Employed |
8 (12.8) |
4 (6.4) |
11 (17.5) |
3.4 (2) |
|
Unemployed |
10 (15.8) |
16 (25.4) |
14 (22.2) |
||
|
ICD-10 |
F2 |
12 (19.1) |
15 (22.7) |
14 (22.2) |
4.8 (6) |
|
F3 |
3 (4.8) |
1 (1.6) |
3 (4.8) |
||
|
F4+F6 |
1 (1.6) |
2 (3.2) |
6 (9.6) |
||
|
F0 |
2 (3.2) |
2 (3.2) |
2 (3.2) |
||
Note: * p ≤0.05; ** p ≤0.01; *** p ≤0.001.
Table 2. Psychometric characteristics of patients with psychotic disorders (F2, F06)
|
Characteristics |
Prevalence in Cluster, N(%) |
χ2(df) |
|||
|
Cluster 1, n=14 |
Cluster 2, n=17 |
Cluster 3, n=16 |
|||
|
BPRS |
≥60 points |
2 (4.3) |
3 (6.4) |
5 (10.6) |
2.2 (4) |
|
40–60 points |
9 (19.1) |
11 (23.4) |
8 (17.0) |
||
|
≤40 points |
1 (2.1) |
2 (4.3) |
3 (6.4) |
||
|
SANS |
≥60 points |
6 (12.8) |
6 (12.8) |
1 (2.1) |
9.9 (4)* |
|
30–60 points |
4 (8.5) |
6 (12.8) |
5 (10.6) |
||
|
≤40 points |
2 (4.3) |
4 (8.5) |
10 (21.3) |
||
|
GAF |
≤40 points |
4 (8.5) |
6 (12.8) |
3 (6.4) |
13.2 (4)** |
|
40-60 points |
7 (14.9) |
9 (19.1) |
4 (8.5) |
||
|
≥ 60 points |
1 (2.1) |
1 (2.1) |
9 (19.1) |
||
Note: * p ≤0.05; ** p ≤0.01; *** p ≤0.001.
Characteristics of internalized stigma and treatment motivation in patients' clusters
According to ANOVA with post-hoc tests, 18 patients in Cluster 1 (29% of the sample) had higher levels of total IS score (Mean dif.=0.90, S.E.=0.089, sig. <0.001) due to a higher level of alienation (Mean dif.=1.20, S.E.=0.17, sig. <0.001), stereotype endorsement (Mean dif.=0.81, S.E.=0.14, sig. <0.001), social withdrawal (Mean Dif.=1.09, S.E.=0.14, sig. <0.001), and discrimination experience (Mean dif.=1.09, S.E.=0.17, sig. <0.001) compared to 25 subjects from Cluster 3 (40% of the sample). The features of stigma structure in Cluster 1 was defined as an “explicit” self-stigmatization.
Twenty patients from Cluster 2 (32% of the sample) were more self-stigmatized (Mean dif.=0.71, S.E.=0.09, sig. <0.001) compared to subjects from Cluster 3 due to a lower level of resistance to self-stigmatization (Mean dif.=-0.71, S.E.=0.17, sig. <0.001). The stigma subtype of Cluster 2 patients was defined as an “implicit” stigma.
Cluster 2 patients demonstrated the lowest treatment motivation compared to the subjects in Clusters 1 and 3 (Mean dif.=-1.53, S.E.=0.20, sig. <0.001; Mean dif.=-1.14, S.E.=0.19, sig. <0.001) due to the lowest TMAQ factor 1 (reliance on one’s own knowledge and skills to cope with the disorder; Mean dif.=-1.67, S.E.=0.22, sig. <0.001; Mean dif.=-1.31, S.E.=0.21, sig. <0.001) and factor 4 (willingness to cooperate with the doctor; Mean dif.=-1.19, S.E.=0.29, sig.=0,01; Mean dif.=-1.13, S.E.=0.26, sig. <0.001).
Explicitly and implicitly stigmatized patients differed from each other in TMAQ factor 3 (awareness of the psychological mechanism of maladjustment), which was lower in the implicitly stigmatized group (Mean dif.=-1.05, S.E.=0.27, sig.=0,01).
DISCUSSION
In this study, the cumulative proportion of patients with psychiatric disorders who had pronounced IS was 60%, which is higher than the prevalence of psychological demoralization reactions (24%) known for patients with non-psychiatric disorders [3].
Three clinically different manifestations of psychiatric stigma internalization with bearing on treatment motivation were observed in a sample of psychiatric inpatients. This result confirmed the first hypothesis about the existence of psychiatric patients capable of withstanding stigma by building a specific structure of treatment motivation.
The most favorable type of reaction to mental disorders was found in the largest portion of the sample with minimal self-stigma measured by ISMI and a favorable treatment motivation structure measured by TMAQ (Cluster 3, 40%). Patients in Cluster 1 (29%) and Cluster 2 (32%) displayed effects of alienation, stereotype endorsement, social withdrawal, and discrimination experiences according the ISMI scale. Nonetheless, patients in Clusters 1 and 2 displayed different health-related behavior due to the differences in treatment motivation.
Patients from Cluster 1 could withstand stigma thanks to cooperation with doctors and reliance on their own knowledge and skills in coping with their illness (according to TMAQ). Therefore, because of the ability of patients in this cluster to show good coping skills in the treatment process, we called self-stigmatization in that category of psychiatric inpatients “explicit self-stigmatization.”
Patients in Cluster 2 exhibited the highest scores on the reversely coded stigma resistance subscale of ISMI. As a result, they passively accepted the role of “mentally ill person” and showed minimal treatment motivation, which was confirmed by the results on the TMAQ scale — patients showed the lowest intensity of treatment motivation and low awareness of the psychological mechanism of maladjustment. Therefore, because of the absence of any active pushback against internalization of stigma, patients in this cluster were categorized as “implicitly self-stigmatized.”
The levels of morbid maladjustment and negative symptomatology (according to the GAF and SANS scales, respectively) in patients with schizophrenia, organic mood (with manic features), and schizophrenia-like disorders in Cluster 1 and Cluster 2 were comparable. They displayed pronounced negative symptoms (SANS score over 60 points) and moderate negative symptoms (SANS score between 40 and 60 points). Social maladjustment was predominantly characterized by moderate levels of GAF scores (scoring between 40 and 60 points). Patients from Cluster 3 had rare maladjustment according to the GAF scale and a low prevalence of negative symptomatology on the SANS scale. The number of patients with schizophrenia, organic mood (with manic features), and schizophrenia-like disorders was comparable in Clusters 1, 2, and 3. Therefore, this result partially confirms the second hypothesis of the study: differences in clinical characteristics among patients with different types of stigmatization are apparent between self-stigmatized (Cluster 1 and Cluster 2) and minimally-stigmatized (Cluster 3) patients, but not between patients with two types of IS with or without lack of treatment motivation (Cluster 1 and Cluster 2). This finding is in accordance with a large body of evidence showing that reducing self-stigma in psychiatric rehabilitation work not only comes with an increase in compliance, but also with symptomatic improvement [22] and reductions in social maladjustment [13].
The two subtypes of stigmatized patients (Clusters 1 and Cluster 2) had differences in clinical and sociodemographic characteristics. Cluster 1 (comprising individuals motivated for treatment and experiencing stigmatization) included older patients with longer illness duration and repeated hospitalizations. The most vulnerable group were the patients from Cluster 2 who, unlike patients from Cluster 1, had IS without building intensive treatment motivation. These patients were younger, they had a shorter duration of the illness, fewer hospitalizations, and were predominantly male.
Strengths and limitations
There are several limitations in this study. The first limitation is the sample size. However, pilot studies in the field of the stated topic quite often rely on small samples: out of the 111 articles included in review [23], around 15% had comparable or smaller sample sizes. The second limitation is the cross-sectional, rather than longitudinal, design of the study, which creates a need to confirm the identified patterns in further observational studies.
The observational nature of this study also determines the nosological heterogeneity of the sample, which, nevertheless, reflects the natural appeal for inpatient psychiatric care at the National Medical Research Centre and is quite common in studies on the psychology of the treatment process [4, 9, 10].
A significant general methodological limitation is the uncertainty of the construct of IS or self-stigma. In this regard, we applied one of the most widely used psychometric tools (ISMI), due to its prevalence, known to be a consensus method of assessing the stigma phenomenon [16]. The literature also describes substantial differences in the prevalence, perception, and internalization of psychiatric stigma across cultures [5]. This underlines the relevance and necessity of expanding transcultural research initiatives into the psychological responses of people with mental illness, with the aim of identifying universal protective factors in relation to self-stigma.
The primary strength and central practical outcome of this study lie in the identification of individuals exhibiting implicit self-stigma (Cluster 2), revealing notably reduced treatment motivation within the realm of all self-stigmatized patients. These observations, detached from disparities in nosology or positive symptomatology between Cluster 2 patients and those categorized in the other two groups (Clusters 1 and Cluster 3), emphasize the potential impact of patients’ personal traits and the disease course on the internalization of stigma. Further research into the psychological mechanisms and clinical factors driving the self-stigmatization phenomenon, especially in terms of motivated and nonmotivated treatment attitudes, holds the promise of forging more tailored and person-centered approaches in the psychiatric rehabilitation of individuals with severe mental disorders.
CONCLUSION
Three clinically different types of reaction to mental disorders were observed in a sample of psychiatric inpatients, which enabled us to identify different psychiatric self-stigmatization subtypes, depending on the type of treatment motivation. The tendency of patients with psychiatric disorders to develop self-stigma is associated with a more pronounced morbid maladjustment and severe negative symptoms, but not positive symptoms. The formation of a favorable or less favorable subtype of IS is mediated predominantly by the disease course and the patients’ gender, but not diagnosis and symptoms severity. Identification of transnosological phenomena such as stigma and motivation toward psychiatric treatment affords us a promising opportunity to develop a personal, rather than nosologically oriented, approach (personalized approach) to patient rehabilitation. Two subtypes of psychiatric stigma were identified depending on health-related behavior. The “explicit” subtype of self-stigmatization can be considered more favorable than the “implicit subtype,” due to a constructive type of treatment attitude with intensive therapeutic motivation among patients with explicit self-stigmatization.