INTRODUCTION
Autism spectrum disorder (ASD) is commonly understood through spectrum-based models, designed to explain the phenotypic and symptomatic variability of the condition. While descriptively effective, these models often fail to capture the underlying functional and adaptive dynamics, particularly those related to sensorimotor integration and the development of bodily self-awareness.
This article introduces an alternative theoretical model, the Bipolar Tensile Model (BTM), developed within a neurosemiotic and informational framework. In this perspective, ASD is not viewed as a collection of traits or deficits, but as the result of an unresolved tension between two complementary hemispheric cognitive styles — symbolic-sequential and corporeal-perceptual — that, in neurotypical conditions, are harmonized by an interhemispheric system of integration.
When this mediation is unstable or ineffective, polarized cognitive patterns may emerge, leading to atypical functional profiles. In this model, proprioception plays a key role, not merely as a peripheral sensory channel, but as an indicator of coherence between cognitive systems and the efficiency of interhemispheric integration.
Despite the growing use of sensory and psychomotor approaches in ASD interventions, proprioceptive integration often remains limited, especially in high-functioning individuals. The proposed model provides an alternative framework for interpretation, suggesting that therapeutic efforts should focus on restoring postural and interhemispheric balance through proprioceptive stimulation, embodied narrative techniques, and integrative hemispheric training.
THEORETICAL FRAMEWORK
Neurosemiotic foundations
The hypotheses presented here draw upon two significant theoretical traditions. Yuri Lotman’s neurosemiotic framework, developed from his seminal work “Culture as collective intelligence and the problem of artificial intelligence” [1], interprets cerebral asymmetry not merely as a biological fact, but as an epistemic structure of culture itself. The two cognitive hemispheres — logical-verbal and visual-holistic — operate through distinct codes and generate meaning through their confrontation and mutual tension. In this view, cultural and cognitive creativity emerges at the boundaries where these divergent systems meet and interact.
Giulio Tononi’s Integrated Information Theory (IIT) [2] posits that consciousness emerges from the highest possible integration among highly differentiated systems. This view also reveals a structural paradox: the greater the specialization (and therefore asymmetry) of the systems involved, the greater the need for global mediation to prevent experiential fragmentation.
Hemispheric specialization and cognitive tension
The BTM places this tension at its core between differentiation and integration as its central organizing principle: cognitive and identity coherence arise from an unstable and dynamic equilibrium between specialized hemispheric poles, continually modulated through proprioceptive and embodied processes.
Although not directly derived from the work of Nikolai Bernstein [3], the model aligns closely with his conception of movement as a centrally regulated, goal-oriented activity. Bernstein’s distinction between anticipatory coordination and retroactive adjustment reflects a functional tension like that proposed here between conscious proprioception and motor automatism. From this perspective, the sensorimotor disturbances observed in ASD may not result from simple executive deficits, but from imbalances between these regulatory systems.
This view is consistent with recent models of distributed brain function, which conceptualize lateralization not as a static division of labor, but as a dynamic axis of specialization and integration — mediated by interhemispheric structures and the Default Mode Network (DMN).
METHODS
This study adopts a theoretical approach to construct an interpretative model that integrates neuroscientific evidence, clinical data, and semiotic perspectives. Its aim is to outline a heuristic framework for understanding the atypical cognitive and sensorimotor dynamics observed in ASD, with a particular focus on proprioception and interhemispheric connectivity.
The BTM was developed through a narrative review of the scientific literature to identify theoretical, clinical, and experimental contributions relevant to the model’s core hypothesis. The literature search included peer-reviewed articles indexed in major international databases (PubMed, Scopus, PsycInfo), without rigid temporal restrictions, to include foundational studies on motor control and hemispheric lateralization. The main keywords used were: “ASD”, “proprioception”, “hemispheric connectivity”, “interhemispheric integration”, “default mode network”, “motor planning”, “sensorimotor integration”, and “semiotics”.
The inclusion criteria prioritized studies that:
- presented neuroimaging data (fMRI, DTI, EEG);
- included sensorimotor evaluations of individuals with ASD;
- explicitly addressed functional lateralization, motor regulation, or body perception.
A central element of the model is the concept of the Extended Default Mode Network, which encompasses not only the cortical areas of the classical DMN, but also the primary interhemispheric commissures (corpus callosum, anterior and hippocampal commissures) and the cerebellum, conceptualized as active nodes of cognitive compensation and integration.
The theoretical framework acknowledges the simplifications required when modeling a multifactorial condition such as ASD: other sensory or cognitive systems not directly related to proprioception have been intentionally omitted to maintain focus on the tensile dynamics of hemispheric processing. The model’s heuristic validity is illustrated through three illustrative clinical cases drawn from the literature, each showing convergence between proprioceptive dysfunction, interhemispheric disconnection, and atypical neurofunctional profiles.
THE BIPOLAR TENSILE MODE
Interhemispheric disconnection and compensation
Numerous neuroimaging studies suggest that ASD is characterized by an atypical pattern of brain connectivity, with increased local intrahemispheric connectivity and reduced communication between homologous interhemispheric regions. These patterns are observable through fMRI, DTI, EEG, and MEG analyses. A significant reduction in interhemispheric connectivity, associated with social interaction deficits, has been reported [4]. Widespread alterations in functional brain connectivity have been confirmed using the ABIDE dataset [5]. A model based on local hyperactivity and weak global integration has been proposed [6], and reduced interhemispheric synchronization and more idiosyncratic processing styles have also been reported [7].
These dysfunctions support the hypothesis that each hemisphere processes information relatively independently, according to its own computational style. Local hyperconnectivity may thus be interpreted as a compensatory strategy, in which each hemisphere reinforces its internal coherence to compensate for weak bilateral integration. Within this dynamic, divergent cognitive profiles emerge: the left hemisphere favors symbolic-sequential processing, while the right hemisphere adopts corporeal-perceptual modes [8–10].
Based on this evidence, the BTM, rooted in semiotic-informational theory, views the heterogeneity of ASD as arising from a functional tension between two complementary cognitive modalities (Figure 1). The “bipolar” axis refers to the deviation from a dynamic equilibrium between hemispheric specializations. When interhemispheric connectivity weakens, each pole tends to amplify its characteristic processing style, leading to polarized cognitive patterns. Clinically, these configurations may manifest as operational rigidity, perceptual selectivity, motor stereotypies, or sensory disorganization.
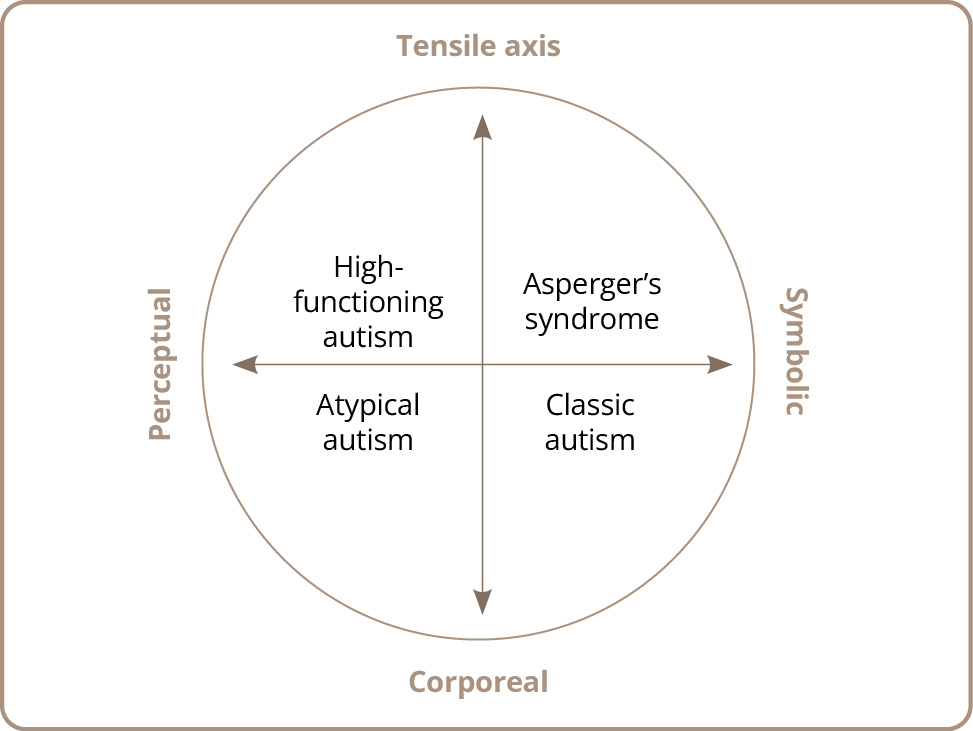
Figure 1. Axial representation of the Bipolar Tensile Model.
Source: Tensile Axis Image concept by M. Sanna, generated by ChatGPT (OpenAI, 2025).
Inspired by the neurosemiotics of Lotman [11] and IIT [2], the model proposes that cognitive lateralization is a plastic and dynamic process. The center of the axis represents a point of active tension in which the two hemispheres seek to integrate qualitatively distinct forms of processing. Hemispheric tension is not pathological per se, on the contrary, it can fuel cognitive creativity and coherence of self. It becomes clinically relevant only when integration fails, resulting in unbalanced profiles, such as disembodied verbalizations or disorganized motor behavior.
The model distinguishes between two semiotic modalities: the left hemisphere operates through discrete codes (analytical, symbolic, sequential), whereas the right hemisphere relies on continuous codes (perceptual, spatial, affective). These cognitive languages, though qualitatively divergent, are potentially integrable via a mediating function.
From this perspective, position along the tensile axis does not represent a rigid clinical typology, but rather indicates a degree of compensation in relation to the prevailing mode. For instance:
- a left-dominant profile may exhibit advanced linguistic abilities with pragmatic rigidity [12, 13];
- a right-dominant profile may be associated with sensory hypersensitivity and hyperverbality [14, 15].
The weaker the interhemispheric communication, the greater the profile’s polarization. Conversely, effective integration of cognitive styles promotes flexibility and self-coherence, even in neurotypical individuals, who are not necessarily centered on the axis, given the high variability of functional asymmetry across individuals.
The compensatory instance
Within the framework of the BTM, we propose the existence of an intermediary neural function, a true mediating mechanism, that not only relay information between hemispheres, but actively regulates their functional tension, acting as a dynamic regulator between qualitatively distinct cognitive styles.
The main challenge of this mediation lies in the asymmetry of hemispheric codes: the left hemisphere processes information in discrete, segmented, and sequential formats; the right hemisphere, by contrast, operates through continuous, spatial, affective, and perceptual configurations. Integrating these heterogeneous cognitive languages requires an active process of recoding rather than direct translation.
Under neurotypical conditions, this mediating function supports adaptive plasticity, which supports the emergence of a coherent and flexible embodied self. In atypical profiles, such as in ASD, this mediation may prove unstable or inefficient, promoting cognitive and sensorimotor fragmentation.
This compensatory mechanism can be understood as an internal regulator of functional coherence, whose purpose is to optimize integration according to an individual’s neurofunctional profile. Anatomically and functionally, the cerebral commissures are the primary structures likely to fulfill this role, primarily the corpus callosum, followed by the anterior and hippocampal commissures. These structures do not merely transmit signals: they modulate, filter, and transform information, actively contributing to the construction of cognitive unity.
As noted by Gazzaniga [16], the corpus callosum is essential for integrating interhemispheric consciousness; van der Knaap and van der Ham [17] further emphasize its selective and integrative function, well beyond simple information transfer.
Parallel research has associated disturbances in the DMN with impairments in self-integration in individuals with ASD. The DMN, comprising the medial prefrontal cortex, precuneus, posterior cingulate cortex, and limbic areas, plays a central role in self-representation and monitoring bodily intentions [18]. A meta-analysis by Wang et al. [19] identified systematic alterations in resting-state DMN connectivity in ASD populations. Similarly, Yao et al. [4] reported reduced connectivity within DMN regions, associated with social deficits. He et al. [20] described topological changes in the network, affecting emotional regulation and behavioral adaptation.
Within interhemispheric mediation, the inferior parietal lobule (IPL) functions as a multisensory hub constructing the body schema. Under conditions of hemispheric disconnection, the IPL becomes vulnerable, disrupting the alignment between perception, intention, and action [21].
The anterior commissure connects limbic and temporoparietal areas and may influence sensory-affective coherence. The hippocampal commissure, involved in memory processing and autobiographical space, is part of both the limbic system and the Extended Default Mode Network, making it an integral component of this mediating mechanism.
This “third structure” can therefore be identified as a functionally integrated system comprising the Extended Default Mode Network and the major cerebral commissures. Together, these constitute the neurofunctional platform of hemispheric compensation.
In individuals with ASD, this integrated network is frequently compromised. Converging studies report reduced connectivity between DMN nodes and structural alterations in the cerebral commissures [22, 23]. This disconnection impairs interhemispheric coherence, resulting in asymmetrical management of information between the symbolic and perceptual poles. Clinically, this produces a persistent tensile imbalance, manifesting as sensorimotor disintegration, repetitive behaviors, and disturbances in the narrative construction of the self.
Within our model, dysfunction of the third structure compromises the system’s central regulatory function, impeding the dynamic balance between complementary cognitive codes.
The heuristic potential of the BTM becomes particularly evident in this configuration: each new clinical profile is read not as a direct product of lesion or dysfunction, but as an adaptive trajectory along the tensile axis.
However, empirical validation of the model requires a cumulative and multidisciplinary approach. The model relies on adaptive axial logic rather than rigid typologies. Its application may initially target documented subgroups (e.g., individuals with marked lateralization or proprioceptive instability) and evolve alongside accumulating clinical and neurofunctional data. Its open structure enables continuous refinement, in line with the increasing complexity of scientific evidence.
IMPAIRMENT OF THE PROPRIOCEPTIVE SYSTEM
Conscious proprioception and automatic kinesthesia
Proprioception — a core function of the sensorimotor system — is not fully operational at birth. It develops gradually through embodied experience, following a trajectory that is initially lateralized and later integrated through interhemispheric transfer into a unified and conscious perception of the self in action [24]. This developmental path parallels Bernstein’s distinction between anticipatory coordination and retroactive adjustment in motor control, which is also applicable to proprioceptive maturation [3].
Within the BTM, we propose, for heuristic purposes, a distinction between two functional modes of the sensorimotor system:
- conscious proprioception is the reflective and intentional perception of the body in action, corresponding to the body image described by Gallagher [25] and associated with analytical, linguistic, and representational functions;
- automatic kinesthesia is a form of embodied, fluid, and non-verbalized action regulated by sub-threshold proprioceptive, vestibular, and somatic signals. This corresponds to Jeannerod’s motor intentionality [26] and Bernstein’s implicit dynamic models [3].
This distinction is not intended to replace computational frameworks such as predictive coding, but instead offers an operational perspective for describing cognitive tensions involved in the self-regulation of bodily experience. It is also essential to understanding the dynamic role of the DMN, which is preferentially active during states of bodily automation and supports the narrative and interhemispheric integration of the self.
In neurotypical individuals, these two modes alternate fluidly, the body acts automatically while the DMN prepares subsequent action sequences. In novel or complex situations, the right hemisphere guides action planning, once the movement is stabilized, the left hemisphere automatizes and consolidates the movement. This cycle ensures motor fluidity, postural coherence, and identity continuity.
In individuals with ASD, this alternation is often disrupted: transitions between control and automation are often incoherent or blocked, manifesting clinically as motor hypercontrol, stereotypies, clumsiness, or unmodulated sensorimotor regressions. Such patterns reflect unregulated tension between misaligned hemispheres, leading to failures in voluntary planning and the emergence of repetitive, non-intentional behaviors.
Neurofunctional studies indicate that individuals with ASD (in the presence of interhemispheric disconnection) often compensate for instability with excessive reliance on visual feedback, at the expense of proprioceptive modulation [27, 28]. This results in postural-tonic alterations, disorganized movement, and repetitive behaviors, interpretable as bodily attempts to stabilize an unstable or fragmented self [14, 29].
Numerous studies now support the central role of proprioception in a wide range of motor and cognitive processes [30, 31]. It is involved in both anticipatory (feedforward) and retroactive (feedback) regulation of movement, and is essential for motor learning, spatial planning, and environmental adaptation [32, 33].
In addition to its motor functions, proprioception also contributes to spatial working memory by providing dynamic representations of the body and its environment [34, 35]. Impairments in this system affect muscle tone, posture, and movement fluidity, with significant effects on daily functioning [36–39].
Distortions in spatial estimation and trajectory prediction disrupt interaction with the environment, often leading individuals on the spectrum to engage in motor stereotypies, such as rocking or rhythmic movements, interpreted here as self-regulatory strategies aimed at re-establishing a minimal sense of bodily perceptual continuity [40].
Within the BTM, such behaviors are understood not as secondary symptoms but as central indicators of a systemic imbalance between conscious proprioception and automatic motor execution — a persistent tension between the poles of anticipation and action.
Poetic language as tensile synthesis: a semiotic analysis of the autistic body
Within the clinical framework of ASD, it is often observed that individuals present an uneven developmental profile, in which gross motor functions appear clumsy or unstable, while fine abilities, such as drawing, writing, or verbal composition, are remarkably well developed. This asynchrony, often dismissed as a functional paradox, can be reinterpreted through the lens of the BTM as the result of localized hemispheric compensation: the hyperfunctional left hemisphere attempts to counter proprioceptive instability by reinforcing symbolic-discrete structures capable of containing disorganized perceptual experience.
Proprioceptive deficiency manifests as a loss of axial alignment, hyporeactive posture, misalignment between intention and action, compensatory visual dependency, and an inability to adapt to new situations fluidly, which must be reconstructed each time, as if the body lacked a memory of experience. In these cases, sensory input fails to integrate into an embodied narrative, fragmenting instead into discontinuous episodes unanchored from the self.
Within this framework, expressive texts produced by individuals with ASD, whether graphic, verbal, or gestural, should be understood not merely as aesthetic exercises, but as attempts at symbolic stabilization. Highly detailed drawings, for instance, reflect an analytical compensatory strategy in response to a deficit in bodily anchoring; meticulous repetition of forms, strict segmentation of space, and focus on isolated elements all serve to reestablish perceptual control.
An emblematic example of proprioceptive and affective self-awareness in neurodivergent writing is Benjamin Giroux’s poem “I Am Odd, I Am New” (2016)[1], composed when the author was ten years old.
The poem captures the embodied perception of difference and the oscillation between vulnerability and affirmation:
I am odd, I am new,
I wonder if you are too.
I hear voices in the air,
I see you don’t, and that’s not fair.
I feel like a boy in outer space,
I touch the stars and feel out of place.
I worry what others might think,
I cry when people just don’t link.
I am odd, I am new,
I understand now that so are you.
I say I “feel like a castaway”,
I dream of a better day.
I try to fit in, I hope that I do,
I am odd, I am new.
This text has been widely circulated as an authentic expression of autistic self-perception and proprioceptive dissonance, illustrating how internal bodily awareness (oddness, spatial dislocation, tactile imagery) becomes linguistic rhythm and poetic identity.
The poem’s graphic layout, with the vertical alignment of the repeated “I am”, visually evokes an ordering structure, functioning as a symbolic sensory axis functioning as a symbolic sensory axis that compensates for the absence of a proprioceptive one. A semiotic analysis of the text reveals sensory dysfunctions typical of ASD: “I hear voices in the air” expresses non-localized auditory hypersensitivity, lacking spatial anchorage; “I touch the stars and feel out of place” reflects a dissociation between tactile contact and proprioceptive feedback, where touching does not coincide with feeling grounded; “I feel like a boy in outer space” encapsulates a profound corporeal delocalization — a loss of narrative gravity and embodied weight.
The poem does not merely describe an emotional state but symbolically encodes a fragmented proprioceptive experience, rendering its sensory profile in metrical form. The symmetry of the phrases, the regularity of repetition, and the analytical segmentation of rhythm perform an ordering function, where the body cannot guarantee continuity, poetic form provides symbolic compensation.
In the BTM, such texts, whether poetic, graphic, or motoric, are interpreted as semiotic traces of adaptation: functional devices activated by the subject to cope with hemispheric asymmetry and loss of sensorimotor coherence. These are not merely expressive outputs, but clinically relevant data, capable of revealing deep dynamics of hemispheric polarization and the compensatory strategies employed.
Semiotic analysis of these texts makes it possible to identify cognitive configurations otherwise inaccessible through standard diagnostic tools. It offers a complementary interpretive resource grounded in an embodied reading of meaning. This approach strongly supports the inclusion of a semiotic perspective within clinical and neuropsychological contexts, underscoring the potential of sign theory to render intelligible the disorganized experiential world of autistic embodiment.
The axiality of the body
The poem analyzed in the previous section highlights a key element for the semiotic understanding of ASD: the absence of an internal bodily axis, that is, the lack of a stable perception of one’s own spatial and identity-related positioning.
In the BTM, space is not understood as an objective structure, but as an active construction rooted in sensorimotor experience. The body does not simply occupy space; it generates it, by articulating referential axes, such as up/down, left/right, front/back; coordinates that are not innate but emerge through embodied interaction with the environment.
From the earliest months of life, the infant explores the world through early actions, such as head-lifting or declarative pointing, that imply bodily localization in relation to objects and others. These early acquisitions, which require precise integration of motor intentionality and proprioceptive feedback, can be interpreted, following Bernstein [3], as dynamic outcomes of the progressive interplay between anticipatory control and sensory retroaction. The pointing gesture, a precursor of symbolic communication [41], activates mirror neurons and reinforces the intersubjective dimension of the self [42].
In individuals with ASD, proprioceptive instability impairs the construction of personal space: postural disorganization, alterations in interpersonal distance regulation, gestural rigidity, and difficulties in intercorporeal coordination are frequently observed. Individuals may experience forms of bodily estrangement, such as the sensation of not inhabiting one’s own body or lacking an “internal gravity” [43], which result in disorientation during interactions with the environment and with others [40].
As Merleau-Ponty [44] observed, space is constituted through the body: only a centered body can articulate intention, movement, and meaning. When this internal axis collapses, language itself loses its experiential foundation, becoming detached from action and lived experience.
From this perspective, proprioception is not merely a sensory system, but an embodied semiotic device: it is a condition of possibility for gesture, meaning, and the emergence of the self. In this light, the semiotic analysis of bodily texts, whether verbal, graphic, or behavioral, can meaningfully inform clinical practice, helping to identify the presence or absence of an internal axis and to interpret the symbolic strategies through which individuals attempt to reconstruct embodied centeredness.
TOWARD FUNCTIONAL SYNTHESIS: THE BIPOLAR TENSILE MODEL IN CLINICAL CONTEXT
In light of the conceptual, clinical, and neurofunctional evidence presented thus far, it is now possible to propose an interpretive synthesis. The goal is not to close the theoretical discussion but rather to outline a possible direction, to reframe disparate elements — interhemispheric disconnection, proprioceptive alteration, and DMN dysfunction, within a unified framework capable of highlighting their dynamic interactions. In this sense, the BTM serves as a heuristic tool for understanding how, under conditions of functional disintegration, the brain can generate divergent compensatory strategies which, though adaptive, contribute to the emergence of the atypical profiles observed on the autism spectrum [45].
Regardless of the origin of commissural insufficiency, its effects depend on which hemisphere receives incomplete information. The contralateral hemisphere processes input unilaterally, according to its characteristic computational style, tends to compensate for the imbalance by enhancing local resources [7, 46]. While this mechanism is adaptive, it can foster the development of distinct cognitive and behavioral patterns in ASD [46, 47].
Research on high-risk infants shows that reduced interhemispheric connectivity is associated with increased reliance on local connections as early as the first year of life [48]. Such findings underscore the central role of cerebral plasticity in compensatory adaptation and help to explain the well-known heterogeneity observed across the spectrum.
In this context, proprioception emerges as a bridge between deep neural mechanisms and observable functional manifestations. More than a simple support for motor control, it is essential to intentional planning as well as cognitive and social competence [49]. Interhemispheric disconnection disrupts sensorimotor synchronization, thereby impairing the efficiency of the DMN — a network central to bodily self-integration.
To illustrate the heuristic validity of the BTM, three clinical cases from the literature are presented that consistently demonstrate a nexus between interhemispheric disconnection, proprioceptive alteration, and DMN dysfunction.
Hagemann [50] describes two children with ASD who exhibit pronounced proprioceptive deficits — poor awareness of the moving body, vestibular hyporesponsiveness, and disorganized gestures. Improvements following intensive sensorimotor training highlight the difficulty in transitioning from conscious proprioception to automatic fluidity.
Leisman et al. [51] report a case characterized by marked asymmetry of the corpus callosum and left-hemispheric dominance. The subject exhibits rich linguistic ability yet profoundly disembodied expression — a verbalization process unsupported by proprioceptive grounding, resulting in a disembodied sense of self.
Paquet et al. [39] examined 34 individuals with ASD, and found postural instability, poor spatial awareness, and uncertain lateralization. Functional asymmetry, confirmed by EEG and cognitive assessments, reflects impaired interhemispheric communication.
Together, these cases demonstrate how the interplay between interhemispheric disconnection, DMN dysfunction, and proprioceptive instability generates fragmented neurofunctional configurations that correspond to the tensile poles described in the model. Far from being merely correlative, this triadic configuration offers a coherent interpretive framework for differential analysis across the autism spectrum.
CONCLUSION
The BTM offers an alternative and integrative interpretation of ASD, grounded in the hypothesis that many clinical manifestations emerge from an unmediated functional tension between cognitive hemispheric specializations. Interhemispheric disconnection, dysfunction and proprioceptive dysregulation of the DMN are not viewed as isolated causes, but as interacting elements within a dynamic system governing self-regulation.
On an epistemological level, the model positions proprioception as a primary semiotic channel — crucial for the emergence of embodied consciousness and sensorimotor coherence. This perspective enables a shift beyond the conventional dichotomy between genetic explanations and phenomenological descriptions, drawing attention to the adaptive modes of atypical functioning.
From a diagnostic standpoint, the model promotes careful observation of subtle but significant bodily indicators; gesture quality, postural stability, motor fluidity, and coherence between intention and action. When integrated with neurofunctional tools, such signs may provide valuable insight into patterns of cognitive lateralization and their compensatory strategies.
Therapeutically, mapping an individual’s tensile profile can guide more targeted interventions. In profiles marked by symbolic-verbal dominance, cognitive abilities may be grounded through proprioceptive stimulation and embodied narrative practices. Conversely, in profiles characterized by perceptual-sensorial dominance, symbolic elaboration of sensory experience may be supported.
A specific contribution of this work lies in its integration of a semiotic perspective: the analysis of verbal, graphic, or behavioral texts produced by individuals on the spectrum may reveal perceptual and tensile states that are otherwise unexpressed, uncovering adaptive strategies and meaning-making trajectories inaccessible to standard tests. This supports the inclusion of semiotic theory in clinical and neuropsychological contexts, filling interpretive gaps left by conventional frameworks.
Nonetheless, the model presents several limitations that must be acknowledged.
First, its nature is essentially theoretical and interpretive: it is not derived from original empirical data, and it does not currently rely on standardized assessment instruments. Second, the clinical cases discussed are illustrative rather than statistically representative, and should be interpreted accordingly. Third, the model does not attempt to claim predictive power or diagnostic classification, nor does it provide direct comparisons with other contemporary models of ASD — such as predictive coding frameworks, connectivist models, or cognitive-behavioral typologies. These comparisons lie beyond the scope of the present essay but remain essential for future validation.
Rather than proposing a definitive explanatory system, the BTM serves as a flexible heuristic framework, intended to generate new hypotheses and promote an embodied, context-sensitive understanding of autistic heterogeneity.
Its greatest strength lies in this adaptability: the axial structure of the model makes it possible to represent the spectrum’s variability not as deviation from the norm, but as the outcome of differential hemispheric compensation trajectories. This perspective opens new avenues for the development of interpretive and rehabilitative protocols centered on corporeal and symbolic resources rather than deficit-based metrics.
Ultimately, the BTM serves as a theoretical and clinical framework for orientation, capable of embracing the complexity of autistic functioning and supporting therapeutic practices more attuned to the lived experience of the individual.
1 National Autism Association [Internet]. Barrington (RI): National Autism Association; 2016 May 6. I’m odd, I’m new [Poem published online]. [cited 2025 Jan 14].
Available from: https://www.facebook.com/photo.php?fbid=10154112555864283&id=299524134282&set=a.41931544428
* Facebook (banned in Russia; owned by Meta Corporation, which is designated as extremist in the Russian Federation)