Introduction
The aim of this case report was to investigate the effect of a musical modification of the sensorimotor integrative therapy (SMITh) on the speech development of a boy with speech delay. Speech and language delay is defined as the child's failure to show the language development expected at the chronological age [Wallace, 2015]. The prevalence of isolated speech and language delays (without associated developmental delays, autism spectrum disorder, or intellectual disability) was estimated at 6% among children aged 2–5 years[Siu, 2015; Wallace, 2015] in the United States. In the Czech Republic, these children are often forced to wait until after the 36th month of life to be diagnosed, but the current recommendation in the Czech Republic is to start the intervention earlier [Bytešníková, 2017]. Internationally, various approaches were found to be effective for intervention in children with speech delay [Fricke, 2013; Girolametto; Wake, 2013].
In this paper, the potential of SMITh for intervention in speech delay is explored. SMITh is a Czech neurorehabilitation approach created in clinical practice by phoniatrician M. Kučera and speech therapist K. Fritzlova, when working with children with developmental and communication problems. This approach belongs to the category of sensory-based interventions [Kantor, 2022], as it is based on and the creation of conditions for the integrated activity of individual sensory subsystems and the integration of motor and sensory perception, where motor determines the quality of sensory perception, and vice versa. The training includes stimulating the cerebellar functions (using balance exercises that shape postural reflexes), the ability to perceive the contours and basic axes of the body, training of time perception, and formation of reflexes that allow one to capture, retain, filter, and integrate external signals. According to the knowledge of the authors, there is no evidence about the effect of sensory-based approaches on speech delays, and the evidence concerning the effect of sensory-based approaches on speech development is rare [7; 10–13]. However, based on the empirical experience from clinical practice, children with speech delay could benefit from sensory-based intervention and the theory of sensorimotor integration may explain the therapeutic mechanisms that enable the therapeutic change in these cases. Therefore, we conducted this pilot case study with the aim to investigate the impact of SMITh intervention on the speech of a boy with speech delay. For this study, we used a musical modification of SMITh described by R. Harvánek [Harvánek, 2022].
Methods
Research with a single-case study design was realised to answer these research questions:
- What are the effects of musical SMITh on the frequency of speech production of a child with speech delay?
- What are the effects of musical SMITh on the frequency of conversation between parents and child with speech delay?
In addition, we observed the quality of speech, comprehension, cooperation with therapist/parent, concentration, fine and gross motor skills, self-care, and perception of time (understanding parts of the day and the concepts of yesterday, today, and tomorrow).
The participant was selected from the first author's private therapy practice based on meeting inclusion criteria:
- The child has a diagnosis of speech delay without other serious developmental problems, namely autism or disorders of intellectual development.
- Preschool age (2–5 years).
- Parent cooperates well with therapy and does exercises at least three times a week in the home environment.
Based on these criteria, we have selected a boy that will be named Václav here. He lives with his parents in a complete and functional family with no other sibling. Both parents have a very nice relationship with him. Václav started the intervention at age 3 years and 4 months because of the speech delay diagnosed by the speech therapist. He was born premature (one month early) and manifested small delays in his movement development. He started to crawl in the 8th month, sit in 12th month, and then he started walking around the furniture. His first words occurred in the 12th month.
In the pre-test examination, parents reported a slight delay in gross motor functions (changes legs only when climbing upstairs, intermittent support by hands needed) and in self-care activities. He understood the sequence of activities, but he did not understand the concepts of yesterday, today, tomorrow. A speech-therapist’s examination reports noticeable attention deficit, impulsivity and hyperactivity, and low level of cooperation. Expressive communication included 15–20 words and occasional two-word sentences. His speech understanding is within norm limits (but the examination was challenged by the low level of cooperation of Václav), he is socially very skilled, and is happy among children.
Intervention
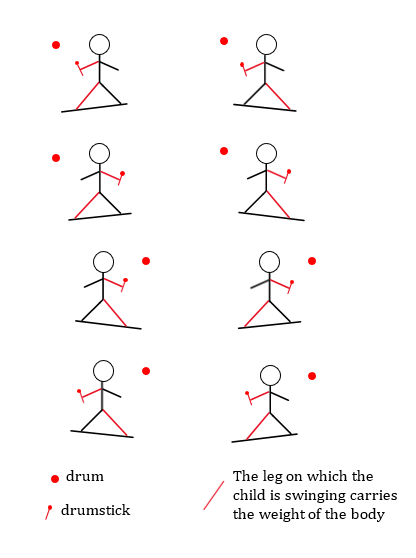
The protocol for musical modification of SMITh included procedures stimulating the tactile sensation of the feet, proprioception with perception of the surface and circumference of the body, perception of the basic vertical axis and other horizontal axes given by paired body parts (inducing postural reflexes) and stimulating connected perception of time and space. In practice, this was done with 11 types of exercises — foot stimulation, body massage with a soft gymnastic ball, outlining the figure of a child, proprioceptive exercises, placing objects on the drawn figure, swinging on a balance board with viewing one-point / pointing to one point / playing a drum, maintaining visual attention on a moving object, spatial hearing, and perception of time with a planning calendar. A detailed description of each activity is attached in supplementary materials (Appendix).
Intervention with the child was conducted for three months, four times a week (once during the music therapy session, and three times at home). One session lasted approximately 45 minutes. All the activities had to be taught continuously and in a playful way, in order of protocol. Throughout the research, we were in contact with the mother at least once a week, either in person or by phone in case of illness and tried to motivate them continuously. As support material, the parents were given a precise description of the individual activities of the sensorimotor integration exercises, a diagram of the exercises on the drum balance board and the necessary equipment. The implementation of the exercises throughout the study was supervised by the author of SMITh.
Outcomes and outcome measures
Primary outcomes (frequency of verbal expressions of child and frequency of communication exchanges between child and parent) were collected during the SMITh exercises using the DLP LENA device (Figure 1), which was placed on the child's chest. The application evaluates the recording and assigns individual sounds into four categories: child vocalizations, adult words, conversational turns of phrase, and environmental sounds. For the research, we looked at two categories — communicative utterances and communicative exchanges between child and parent.
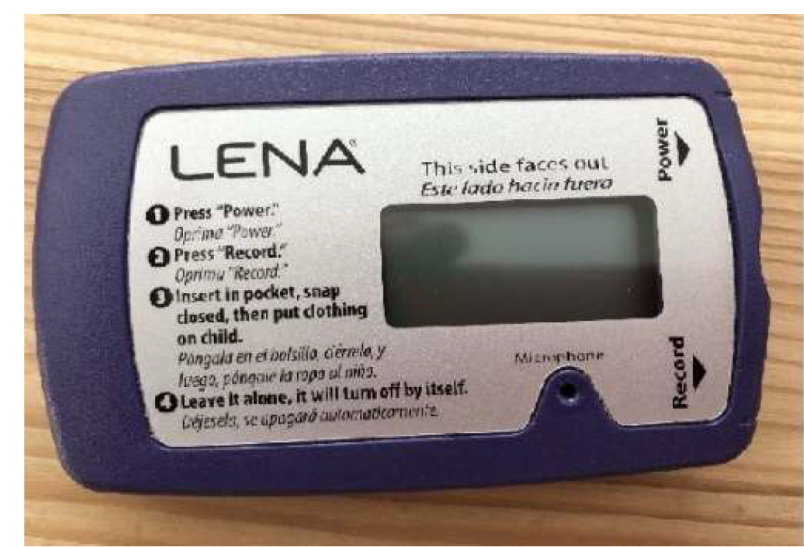
Figure 1. Digital Language Processor LENA
Secondary outcomes were observed using:
- parent interview (once in a week during all the intervention with goals to reflect the course of intervention),
- questionnaire (parents rated on a 0–3 scale the level of gross and fine motor skills, psychomotor restlessness, speech/communication, and perception of time; each item also included an open-ended response option for comments), speech therapist reports from pre-test and post-test phases (comprehension, quality of speech). The questionnaire was filled out before the start of each exercise and then after the end of the exercise,
- parents´ diary — written reflection of each exercise (narratively assessing the course of the exercise and the child's willingness to cooperate, shifts in the quality of verbal communication, understanding, attention and improvement in time orientation, and any other significant changes or events),
- textual analysis of audio recordings of the exercises (quality of speech and content of communication exchanges).
The data analysis was conducted through descriptive statistics and through narrative analysis of textual data. The primary outcomes (data collected through LENA DLP) were graphically processed, assessing the child vocalizations, adult words, conversational turns of phrase. The y-axis of the linear line graph (Figure 2) is based on arithmetic averages of words per minute and captures the progression of 34 measurements (x-axis).
Results
Václav's average verbal expression during the training period ranged from an average of two to fifteen vocalizations per minute, with his mother's frequency between two and ten words per minute and conversational turns of one to five per minute. From the first week of recording, Václav's word count increased, and his mother's word count decreased. By the third month of recording, the child's word count began to clearly outnumber the adult's count. Based on the textual analysis of the audio recordings and the interview with the mother, it was evident that the mother gradually became very tired from the exercises. Therefore, her verbal expression intentionally decreased. She gradually gave the child more space for verbal expression; she deliberately reduced her verbal expression. However, this was not reflected in a change in the number of conversational turns.
The speech therapist´s examination confirmed a growing active vocabulary, as Václav started to speak in longer sentences (combining up to five words). Still, there is worse intelligibility of speech comparing to norm and suspected verbal dyspraxia. Significant progress was reported also in cooperation and longer attention (for more than 30 minutes) by speech therapists. Václav had no tendency to run away from the chair and works well also without his mother’s close presence. According to the parents´ post-post-test report, there is better concentration of attention generally during all activities. He improved in time perception and time orientation — understands the terms yesterday, morning, afternoon, evening, tomorrow and recalls what activities have been planned. According to the parents’ diary, the most significant progress in verbal communication occurred after eight weeks of training. Václav´s mother noted: “Significant shift in speech with speech therapist, repeated words after her. He said more than fifty words on his own. He is already beginning to tell what he did, what he is going to do. He understands the timeline very well in terms of ‘we will go out and have a treat in the afternoon’, he remembers the idea himself and then points it out to me that I promised him.”
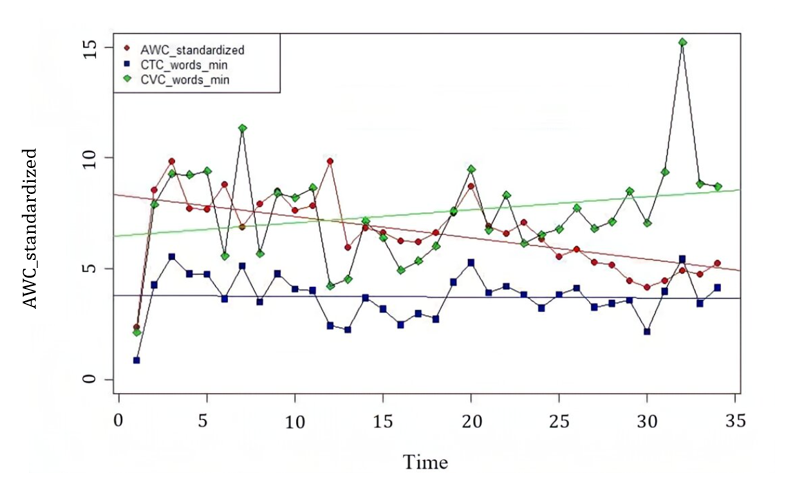
Figure 2. Measurement results of parameters detected by LENA DLP (CVC — child vocalizations, AWG — adult words, CTC — conversational turns of phrase)
Discussion
This first case study exploring the impact of SMITh on the speech of a boy with speech delay found significant improvement of speech production, increase of active vocabulary and creation of longer sentences. The increase of Václav’s speech production compensated a decreased mother´s activity during the conversational turns. Also, progress in attention, cooperation, and time perception was reported by the mother / speech therapists.
These results are easy to explain by the theory of sensorimotor integration. Slight development delays in different areas in Václav prior to intervention signalised immaturity of sensory processing functions [Ben-Sasson, 2009; Chang, 2016] that negatively influenced also motor reactions and development. This case study’s findings correspond to empirical findings from clinical practice of the authors of SMITh, however there was less severe pathology in Václav in comparison to most of the current recipients of SMITh intervention.
Considering short time-period that was needed for gaining such progress of the boy, SMITh could be considered as a therapeutic approach for preschool children with speech delay, especially in case of accompanying developmental problems. The findings of this case study are worthy in the context of international research focused on the impact of sensory-based interventions on speech and communication. There are only rare case studies that explored the impact of sensory-based interventions on spontaneous speech, percentage of vocalisations and other parameters of speech production, mostly in the population of children with autism spectrum disorder or other developmental disabilities [Linderman, 1999; Ray, 1988; Reilly, 1983]. Furthermore, these studies reported mixed results. We found no studies focused on children with speech delay that could benefit from these interventions as well. Sensory-based interventions are mostly applied by occupational therapists, who usually don´t intervene in children with speech delay. Our findings support the idea that speech therapists could be trained in some sensory-based interventions or could cooperate with professionals using these approaches [Lindblom, 2021]. In the Czech Republic, the intervention could be applied by specially trained music therapists, or special teachers, being one of the innovative approaches in rehabilitation [17].
However, the findings must be considered in context of this case study’s limitations. The results could be biased by various factors, e.g., speech therapy intervention that took place during the study, or by spontaneous maturation of the child. Therefore, a trial with a sufficient sample size is needed to prove the effectiveness of SMITh for intervention in speech delays.
Conclusion
This first case study exploring the impact of SMITh on speech delay found positive results in speech production, attention, cooperation, and time perception in a preschool boy with speech delay and slight other developmental problems. There is rationale to consider the usage of this intervention in clinical practice, but future research (optimally a trail with sufficient sample size) is needed to prove the effectiveness of SMITh and its potential for the population of children with speech delay.