INTRODUCTION
Eating disorders, including anorexia nervosa and bulimia nervosa, are associated with a broad array of disruptions in psychological functioning, which, along with symptoms of eating disorder, can uniquely negatively affect quality of life across multiple domains [1, 2]. Two of the most studied psychological phenomena to date that accompany eating disorders are low self-esteem and depressive symptoms. Low self-esteem has been identified, for example, as an important risk factor in the development and persistence of eating disorders [3, 4] and is linked to poorer outcomes [5]. Depressive symptoms (e.g., low mood, loss of interest or pleasure in life activities, unjustified feelings of guilt, etc.) have similarly been linked to poorer outcomes for people with eating disorders [6, 7].
While this research has painted a richer picture of how low self-esteem and depressive symptoms are linked to poor quality of life over time in cases of eating disorders, it is less clear whether these relationships are affected by other psychological variables. As such, work is needed to search for potential determinants of these relationships in people with eating disorders in order to better understand the causal roots of poor quality of life and identify potential mechanisms which could be targeted by treatment.
One potential set of psychological processes that might affect the relationships between self-esteem, depressive symptoms, and quality of life involves metacognition. Metacognition in general refers to the process of thinking about, monitoring, and adjusting one’s own thoughts, and can include attitudes about habitual thought processes, error monitoring, as well as forming an integrated sense of oneself and others [8]. As research has evolved, it has been suggested that metacognitive processes underlie not just how persons choose to take discrete actions, but also allow persons to form a larger and evolving sense of themselves and others as unique persons in the world [9]. Following this, deficits in metacognition, in particular those that manifest in difficulties forming an integrated sense of self or others, have been suggested to represent a transdiagnostic phenomenon which affect quality of life across differing forms of mental disorders, including schizophrenia, depression, bipolar disorder, post-traumatic stress disorder, and personality disorders [2, 10]. This work suggests that metacognitive capacity may have a complex relationship with quality of life, allowing persons to both be aware of the realities of the challenges they face as well as potentially experiencing the devastation of loss [11–13].
Turning to eating disorders, preliminary work suggests that there are impairments in metacognition in these populations [14–17]. Notably, one study found evidence of significant metacognitive deficits which are relatively more severe in anorexia relative to bulimia [18]. The study further indicated that poorer metacognitive capacity was predictive of more severe levels of general psychopathology in bulimia (e.g., positive psychotic symptoms, negative psychotic symptoms, cognitive symptoms, and hostility) and higher levels of disordered eating behavior in anorexia. This finding raises the possibility that metacognitive abilities in eating disorders may similarly influence quality of life, as they do in other conditions, which may potentially help us in understanding how self-esteem and depressive symptoms are related to quality of life in general or, more specifically, in one particular form of eating disorders.
To explore this issue, the current study examined whether two domains of metacognition — metacognitive self-reflectivity and metacognitive mastery — play a role in the relationships between self-esteem, depressive symptoms, and quality of life in eating disorders. The first of these domains, self-reflectivity, refers to the ability to identify and distinguish between one’s own mental experiences, including thoughts and emotions, and integrate these experiences in a meaningful way to form increasingly complex ideas about oneself [19]. One way this ability could affect the relationships between low self-esteem, depressive symptoms, and quality of life is that those with higher levels of self-reflectivity might be able to perceive in clearer detail the links between their emotional distress and the general state of their lives. This is consistent with the results of work done among people with obsessive compulsive disorders showing that increased reflection upon one’s cognitive processes can be associated with increased negative appraisals of intrusive thoughts and increased importance placed on these thoughts [20]. This might also be thought to parallel what has been referred to as depressive realism in persons in general or the insight paradox observed in psychosis, in which increased insight results in higher levels of distress [21].
The second metacognitive domain is mastery. Mastery refers to the ability to make sense of psychosocial challenges and then use metacognitive knowledge of oneself and others to decide how to effectively respond to them. While self-reflectivity could enable low self-esteem and depressive symptoms to result in low quality of life, mastery may have the opposite effect. With greater levels of mastery, persons are more likely to be able to make sense of and live with the pain of low self-esteem and depressive symptoms and be able to achieve a relatively higher quality of life. This conclusion has been supported in studies of psychosis indicating that symptoms are less disruptive when mastery is at relatively greater levels [22] and that mastery is related to generally higher levels of quality of life over time [23]. Additionally, both metacognitive self-reflectivity and metacognitive mastery have been identified as moderating variables in other disorders, including schizophrenia-spectrum disorders, bipolar disorders, and major depressive disorders [22, 24].
To explore these questions, we assessed self-esteem, depressive symptoms, metacognitive self-reflectivity, metacognitive mastery, and several aspects of quality of life among adults with two forms of eating disorders: anorexia and bulimia. We chose these two disorders, because while low self-esteem, depressive symptoms, and poor quality of life are prominent features in each, different risk factors and maintenance processes have been identified, and metacognition appears, at least preliminarily, to have different correlates in each disorder [18].
This study had two primary aims. First, we sought to examine whether metacognitive self-reflectivity and metacognitive mastery moderated the relationships between self-esteem and quality of life and depressive symptoms and quality of life. As described above, we had competing hypotheses regarding the role of metacognitive self-reflectivity and mastery in these relationships; thus, we aimed to examine whether self-reflectivity and mastery strengthened or weakened the negative effects of poor self-esteem/experiences of depressive symptoms with quality-of-life outcomes. Second, we aimed to explore whether these relationships would vary between diagnostic groups of anorexia and bulimia.
METHODS
Participants
Participants consisted of adults diagnosed with anorexia nervosa (n=40) and bulimia nervosa (n=40). They were recruited from the outpatient department of Mental-health clinic No. 1 named after N.A. Alexeev via referral from their treating physician. The participants were not eligible if they had ongoing alcohol or drug dependence, neurological disorders, had been hospitalized in the preceding month, or if they were unable to provide informed consent.
Measures
The Metacognition Assessment Scale-Abbreviated (MAS-A) [25] was used to assess metacognitive capacity. MAS-A scores were derived from transcripts of the Indiana Psychiatric Illness Interview (IPII) [26], which is a semi-structured interview that asks participants to describe their life story and their understanding of their mental illnesses. The MAS-A produces a total score, as well as four subscale scores, including self-reflectivity, awareness of the minds of others, decentration, and mastery [19]. For the current study, we focused on the self-reflectivity and mastery subscales, both of which range from 0 to 9. Higher scores on the self-reflectivity subscale suggest a greater ability to think about and integrate one’s own thoughts and emotions in increasingly integrated, as opposed to fragmented, ways. Higher mastery scores in parallel reflect the ability to find increasingly individualized and nuanced ways to understand and respond effectively to psychosocial challenges. This study used a Russian language version of the IPII and the MAS-A, which has been used previously to measure metacognition in Russian samples [27].
The Rosenberg Self Esteem Scale (RSES) [28] is a 10-item self-report measure that assesses global self-worth. Responses are provided on a 4-point Likert scale from strongly agree (4) to strongly disagree (1). The total score is calculated by summing all items. Higher scores indicate better self-esteem.
The Beck Depression Inventory-II (BDI-II) [29] is a 21-item self-report scale that assesses the severity of depressive symptoms. Responses to each item are on a 4-point Likert scale from 0–3, with higher scores indicating more depressive symptoms. An overall score is calculated by summing the ratings for each item (range: 0–63).
The World Health Organization Quality of Life (WHOQOL) [30] questionnaire is a 100-item self-report measure that assesses quality of life across six domains: psychological well- being, physical health, environment, level of independence, social relationships, and spiritual, religious, and personal beliefs. Responses to each item are on a 1–5 Likert scale, with higher values indicating better quality of life.
Procedures
Procedures were approved by the ethics committee of Mental-health clinic No. 1 named after N.A. Alexeev. After securing informed consent, diagnostic clinical interviews were conducted to confirm the diagnoses. Diagnoses were determined according to ICD-10. The IPII, RSES, BDI-II, and WHOQOL were then administered by a trained interviewer. IPII interviews were transcribed and rated by raters trained by the author of the MAS-A (PL). MAS-A raters were blind to other scores. All measures were administered in the Russian language.
Statistical analysis
First, the demographic characteristics and mean scores for each group were examined. Pearson’s R correlations were then conducted to examine bivariate relationships between MAS-A self-reflectivity, MAS-A mastery, RSES, BDI, and WHOQOL domains. The PROCESS macro [31] in SPSS 29.0 was used to conduct a series of moderation models, which were run separately across the two diagnostic groups. The relevant predictor (i.e., RSES or BDI), the moderator of interest (i.e., MAS-A self-reflectivity or MAS-A mastery), and the interaction term between these variables were entered into separate regression models predicting WHOQOL domains (WHOQOL-psychological, WHOQOL-social, WHOQOL-physical, WHOQOL-independence, WHOQOL-environment, and WHOQOL-spiritual). Moderation was deemed present if the interaction term was statistically significant and significantly improved the regression model. Significant interactions were visualized using the pick-a-point approach [32], and the Johnson-Neyman technique [33] was used to ascertain the value of the moderator (MAS-A self-reflectivity or MAS-A mastery) at which relationships between the RSES, BDI, and WHOQOL domains changed in significance.
RESULTS
All participants were female (n=80). The participants were an average of 24.01 years old (SD=5.22) across the sample, and the anorexia (M=23.95; SD=4.87) and bulimia groups (M=24.08; SD=5.60) did not differ in age. Mean scores and correlations are presented in Table 1. MAS-A self-reflectivity was not significantly associated with the RSES, BDI, or WHOQOL domains across diagnostic groups. In the bulimia group, MAS-A mastery was significantly correlated with WHOQOL-physical (r=-35, p=0.03). No other correlations between MAS-A mastery, RSES, BDI, or WHOQOL domain were significant across the diagnostic groups.
Table 1. Means, standard deviations, and correlations by diagnostic group
|
Anorexia (n=40) |
||||||||||
|
Mean (SD) |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
|
|
RSES |
25.08 (3.97) |
|||||||||
|
BDI |
15.05 (10.27) |
-0.21 |
||||||||
|
MAS-A self-reflectivity |
3.31 (0.49) |
0.04 |
0.03 |
|||||||
|
MAS-A mastery |
2.23 (0.48) |
0.09 |
0.02 |
0.29 |
||||||
|
WHOQOL-social |
35.98 (5.03) |
0.51*** |
-0.40** |
-0.22 |
0.06 |
|||||
|
WHOQOL-physical |
40.03 (6.73) |
0.50*** |
-0.43** |
-0.04 |
0.12 |
0.56*** |
||||
|
WHOQOL-independence |
60.38 (10.68) |
0.19 |
-0.14 |
-0.07 |
0.003 |
0.43** |
0.38* |
|||
|
WHOQOL-environment |
96.13 (14.47) |
0.70*** |
-0.33* |
-0.16 |
0.20 |
0.57*** |
0.68*** |
0.38* |
||
|
WHOQOL-spiritual |
14.13 (3.80) |
0.46** |
-0.34* |
-0.14 |
0.22 |
0.54*** |
0.54*** |
0.13 |
0.61*** |
|
|
WHOQOL-psychological |
54.68 (11.74) |
0.54*** |
-0.48** |
0.02 |
-0.07 |
0.59*** |
0.70*** |
0.21 |
0.58*** |
0.53*** |
|
Bulimia (n=40) |
||||||||||
|
Mean (SD) |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
|
|
RSES |
25.28 (6.54) |
|||||||||
|
BDI |
11.75 (9.92) |
-0.19 |
||||||||
|
MAS-A self-reflectivity |
4.11 (0.46) |
-0.22 |
0.13 |
|||||||
|
MAS-A mastery |
3.0 (0.68) |
-0.16 |
0.03 |
0.49*** |
||||||
|
WHOQOL-social |
40.60 (7.38) |
0.18 |
-0.45** |
0.03 |
-0.03 |
|||||
|
WHOQOL-physical |
37.15 (8.54) |
0.23 |
-0.37* |
-0.26 |
-0.35* |
0.33* |
||||
|
WHOQOL-independence |
58.40 (11.06) |
0.06 |
-0.36* |
-0.14 |
-0.28 |
0.16 |
0.62** |
|||
|
WHOQOL-environment |
100.48 (10.84) |
0.34* |
-0.46** |
-0.16 |
-0.13 |
0.39* |
0.57** |
0.46** |
||
|
WHOQOL-spiritual |
14.65 (3.09) |
0.15 |
-0.45** |
-0.14 |
-0.16 |
0.54** |
0.06 |
0.04 |
0.07 |
|
|
WHOQOL-psychological |
60.63 (13.98) |
0.31 |
-0.63*** |
-0.13 |
-0.18 |
0.60*** |
0.63*** |
0.45** |
0.63*** |
0.46** |
Note: ***p <0.001; **p <0.01; *p <0.05. For MAS-A self-reflectivity and MAS-A mastery, higher scores indicate better metacognition. For RSES, higher scores indicate better self-esteem. For BDI, higher scores indicate more severe depressive symptoms. For WHOQOL domains, higher scores indicate better quality of life. RSES=Rosenberg Self Esteem Scale; BDI=Beck Depression Inventory-II; MAS-A self-reflectivity=Metacognition Assessment Scale-Abbreviated — Self-Reflectivity; MAS-A mastery=Metacognition Assessment Scale-Abbreviated — Mastery; WHOQOL-social=World Health Organization Quality of Life — social relationships; WHOQOL-physical=World Health Organization Quality of Life — physical health; WHOQOL-independence=World Health Organization Quality of Life — level of independence; WHOQOL-environment=World Health Organization Quality of Life — environment; WHOQOL-spiritual=World Health Organization Quality of Life — spiritual, religious, and personal beliefs; WHOQOL-psychological=World Health Organization Quality of Life — psychological well-being.
Moderation analyses: self-reflectivity
The results of the moderation analyses for self-reflectivity in the anorexia group can be seen in Table 2. Significant interactions were found in moderation models examining the relationships between RSES and WHOQOL-social, WHOQOL-physical, and WHOQOL-independence. Overall, results indicated that when self-reflectivity was high, lower self-esteem was associated with poorer quality of life. At lower levels of self-reflectivity, these relationships became non-significant. Johnson-Neyman values were similar; for WHOQOL-social, scores at or above 3.06 on self-reflectivity (32.5% of the sample) exhibited a significant relationship, while for WHOQOL-physical, scores at or above 3.13 (32.5%) exhibited a significant relationship. For WHOQOL-independence, scores at or above 3.63 on self-reflectivity (25%) exhibited a significant relationship. Self-reflectivity also significantly moderated the relationship between RSES and WHOQOL-environment. At all levels of self-reflectivity, lower self-esteem was associated with poorer quality of life, but the effect was stronger when self-reflectivity was high. There were no statistically significant transition points found using the Johnson-Neyman technique (see Figure 1 for graphs of these interactions). No significant interactions were found in the models examining the relationships between RSES and WHOQOL-psychological or WHOQOL-spiritual.
Table 2. Results of significant moderations by self-reflectivity in anorexia
|
Anorexia |
||||
|
Variable |
Coefficient |
SE |
t |
p |
|
Self-Esteem Models |
||||
|
WHOQOL-social: R2=0.40, F=7.91, p <0.001 |
||||
|
Constant |
84.73 |
27.16 |
3.12 |
0.004 |
|
Self-Esteem |
-1.67 |
1.09 |
-1.53 |
0.135 |
|
Self-Reflectivity |
-19.12 |
7.84 |
-2.44 |
0.020 |
|
Interaction Term: R2 change=0.08 |
0.68 |
0.31 |
2.16 |
0.037 |
|
WHOQOL-physical: R2=0.37, F=7.12, p <0.001 |
||||
|
Constant |
114.45 |
37.15 |
3.08 |
0.004 |
|
Self-Esteem |
-2.94 |
1.49 |
-1.97 |
0.057 |
|
Self-Reflectivity |
-27.98 |
10.72 |
-2.61 |
0.013 |
|
Interaction Term: R2 change=0.12 |
1.11 |
0.43 |
2.57 |
0.014 |
|
WHOQOL-environment: R2=0.62, F=19.68, p <0.001 |
||||
|
Constant |
233.47 |
62.0 |
3.77 |
<0.001 |
|
Self-Esteem |
-4.90 |
2.49 |
-1.97 |
0.057 |
|
Self-Reflectivity |
-59.04 |
17.89 |
-3.30 |
0.002 |
|
Interaction Term: R2 change=0.10 |
2.18 |
0.72 |
3.04 |
0.004 |
|
WHOQOL-independence: R2=0.17, F=2.49, p=0.07 |
||||
|
Constant |
210.10 |
67.64 |
3.11 |
0.004 |
|
Self-Esteem |
-5.88 |
2.72 |
-2.16 |
0.037 |
|
Self-Reflectivity |
-47.45 |
19.51 |
-2.43 |
0.020 |
|
Interaction Term: R2 change=0.13 |
1.86 |
0.78 |
2.38 |
0.023 |
|
Depressive Symptom Models |
||||
|
WHOQOL-environment: R2=0.21, F=3.24, p=0.03 |
||||
|
Constant |
70.55 |
28.04 |
2.52 |
0.017 |
|
Depressive Symptoms |
2.49 |
1.51 |
1.65 |
0.108 |
|
Self-Reflectivity |
9.68 |
8.36 |
1.16 |
0.255 |
|
Interaction Term: R2 change=0.08 |
-0.88 |
0.45 |
-1.97 |
0.057† |
|
WHOQOL-spiritual: R2=0.23, F=3.58, p=0.02 |
||||
|
Constant |
6.22 |
7.28 |
0.85 |
0.399 |
|
Depressive Symptoms |
0.70 |
0.39 |
1.78 |
0.084 |
|
Self-Reflectivity |
2.93 |
2.17 |
1.35 |
0.185 |
|
Interaction Term: R2 change=0.10 |
-0.25 |
0.12 |
-2.12 |
0.041 |
†Interaction term is approaching significance.
Note: WHOQOL-social=World Health Organization Quality of Life — social relationships; WHOQOL-physical=World Health Organization Quality of Life — physical health; WHOQOL-environment=World Health Organization Quality of Life — environment; WHOQOL-independence=World Health Organization Quality of Life — level of independence; WHOQOL-spiritual=World Health Organization Quality of Life — spiritual, religious, and personal beliefs.
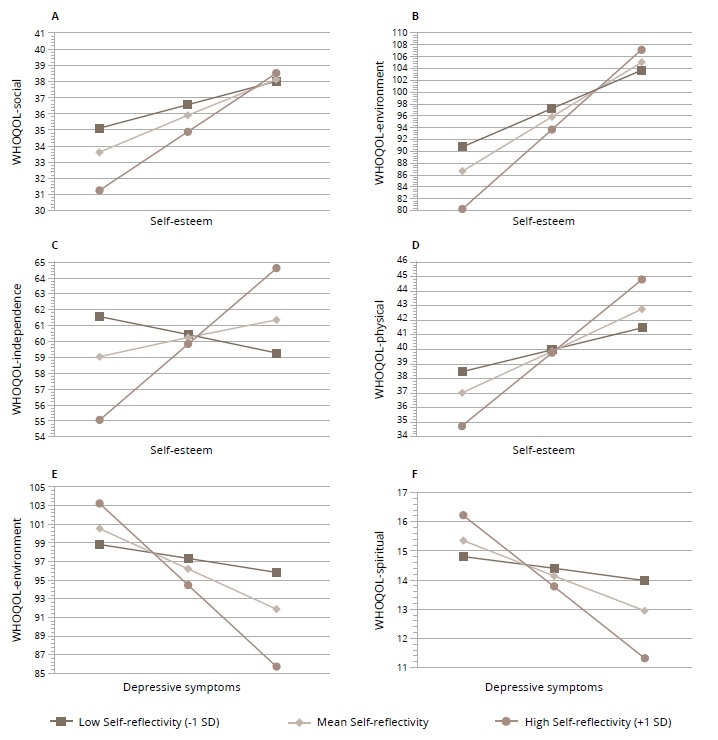
Figure 1. Visualizations of the moderation effect of self-reflectivity on the relationships between self-esteem, depressive symptoms, and quality of life domains (WHOQOL) in the anorexia group.
Regarding depressive symptoms, self-reflectivity significantly moderated the relationship between BDI and WHOQOL-spiritual for those with anorexia (Figure 1). In the model examining BDI and WHOQOL-environment, the interaction term was approaching significance (p=0.057). For both models, when self-reflectivity was high, higher BDI scores were associated with lower WHOQOL scores, while at lower levels of self-reflectivity, relationships were non-significant. For WHOQOL-environment, scores at or above 3.31 on self-reflectivity (32.5%) had a significant relationship, while for WHOQOL-spiritual, scores at or above 3.29 (32.5%) exhibited a significant relationship. Interactions were not significant in the models examining the relationships between BDI and all other WHOQOL domains.
Moderation analyses were repeated for those in the bulimia group. No significant interactions were found in moderation models examining the relationships between RSES and WHOQOL-psychological, WHOQOL-social, WHOQOL-physical, WHOQOL-environment, WHOQOL-independence, or WHOQOL-spiritual. Similarly, no significant interactions were found in the models examining the relationships between BDI and all WHOQOL domains.
Moderation analyses: mastery
The results of the moderation analyses examining mastery can be seen in Table 3. In the anorexia group, mastery significantly moderated the relationship between RSES and WHOQOL-social. When mastery was low, lower RSES scores were associated with lower WHOQOL scores, while at higher levels of mastery, these relationships were non-significant. Johnson-Neyman values indicated that these relationships were significant when mastery scores were at or below 2.27 (75% of the sample). Interactions were not significant in the models examining the relationships between RSES and all other WHOQOL domains. Similarly, no significant interactions were found in the models examining the relationships between BDI and all WHOQOL domains in the anorexia group.
Table 3. Results of significant moderations by mastery in anorexia and bulimia
|
Bulimia |
||||
|
Variable |
Coefficient |
SE |
t |
p |
|
Self-Esteem Models |
||||
|
WHOQOL-physical: R2=0.29, F=4.97, p=0.006 |
||||
|
Constant |
-13.72 |
22.50 |
-0.61 |
0.546 |
|
Self-Esteem |
2.37 |
0.81 |
2.91 |
0.006 |
|
Mastery |
15.07 |
7.30 |
2.06 |
0.046 |
|
Interaction Term: R2 change=0.14 |
-0.72 |
0.27 |
-2.69 |
0.011 |
|
WHOQOL-psychological: R2=0.24, F=3.73, p=0.02 |
||||
|
Constant |
-33.67 |
38.29 |
-0.88 |
0.385 |
|
Self-Esteem |
3.88 |
1.38 |
2.80 |
0.008 |
|
Mastery |
26.45 |
12.43 |
2.13 |
0.040 |
|
Interaction Term: R2 change=0.13 |
-1.11 |
0.46 |
-2.43 |
0.020 |
|
WHOQOL-environment: R2=0.28, F=4.59, p=0.008 |
||||
|
Constant |
15.51 |
28.90 |
0.54 |
0.595 |
|
Self-Esteem |
3.36 |
1.04 |
3.21 |
0.003 |
|
Mastery |
23.86 |
9.38 |
2.54 |
0.015 |
|
Interaction Term: R2 change=0.15 |
-0.95 |
0.34 |
-2.76 |
0.009 |
|
Depressive Symptom Models |
||||
|
WHOQOL-psychological: R2=0.49, F=11.44, p <0.001 |
||||
|
Constant |
101.88 |
12.15 |
8.39 |
<0.001 |
|
Depressive Symptoms |
-2.84 |
0.89 |
-3.20 |
0.003 |
|
Mastery |
-10.56 |
4.05 |
-2.61 |
0.013 |
|
Interaction Term: R2 change=0.07 |
0.67 |
0.30 |
2.26 |
0.030 |
|
Anorexia |
||||
|
Variable |
Coefficient |
SE |
t |
p |
|
Self-Esteem Models |
||||
|
WHOQOL-social: R2=0.36, F=6.89, p <0.001 |
||||
|
Constant |
-21.60 |
17.85 |
-1.21 |
0.234 |
|
Self-Esteem |
2.41 |
0.75 |
3.20 |
0.003 |
|
Mastery |
20.99 |
8.81 |
2.38 |
0.023 |
|
Interaction Term: R2 change=0.10 |
-0.88 |
0.37 |
-2.40 |
0.022 |
Note: WHOQOL-physical = World Health Organization Quality of Life – physical health; WHOQOL-psychological = World Health Organization Quality of Life – psychological well-being; WHOQOL-environment = World Health Organization Quality of Life – environment; WHOQOL-social = World Health Organization Quality of Life – social relationships.
Moderation analyses examining mastery were then repeated in the bulimia group. Significant interactions were found in the models examining RSES and WHOQOL-physical, WHOQOL-psychological, and WHOQOL-environment. For all models, results indicated that at lower levels of mastery, lower self-esteem was associated with poorer quality of life, but when mastery was high, the relationships were non-significant. Johnson-Neyman values were similar across models; for WHOQOL-physical, scores at or below 2.74 (22.5%) exhibited a significant relationship, while for WHOQOL-psychological, relationships were significant for scores at or below 2.93 (22.5%). For WHOQOL-environment, relationships were significant for scores at or below 3.02 (77.5%) on mastery (see Figure 2 for graphs of these interactions). No significant interactions were found in the models examining the relationships between RSES and WHOQOL-independence, WHOQOL-social, or WHOQOL- spiritual.
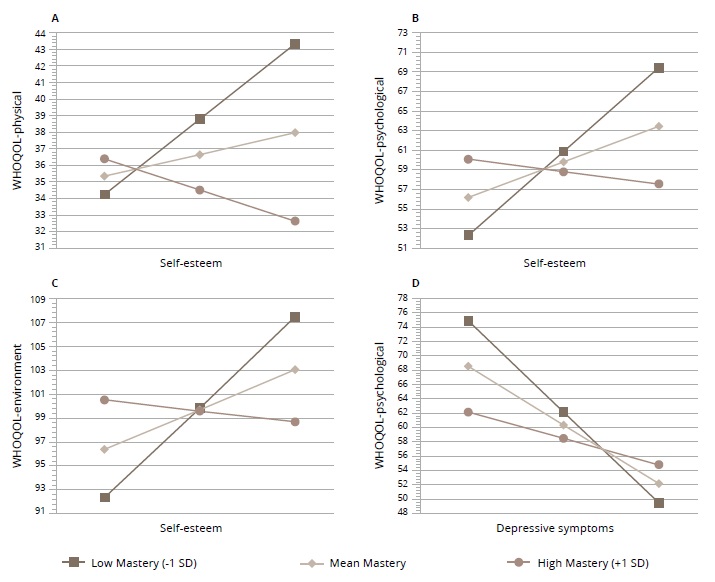
Figure 2. Visualizations of the moderation effect of mastery on the relationships between self-esteem, depressive symptoms, and quality of life domains (WHOQOL) in the bulimia group.
Regarding depressive symptoms, mastery significantly moderated the relationship between BDI and WHOQOL-psychological for those with bulimia (Figure 2). At lower levels of mastery, higher BDI scores were associated with lower WHOQOL scores, while at higher levels of mastery, the relationships were non-significant. Scores at or below 3.51 (77.50%) on mastery exhibited a significant relationship. Interactions were not significant in the models examining the relationships between BDI and all other WHOQOL domains in the bulimia group.
DISCUSSION
This study is the first, to our knowledge, to investigate whether metacognitive self-reflectivity and mastery have an impact on the relationships between self-esteem, depressive symptoms, and quality of life, and whether these impacts vary between people diagnosed with anorexia or bulimia. As expected, metacognitive self-reflectivity and metacognitive mastery had contrasting moderating relationships between the eating disorder groups. In the anorexia group, as expected, self-reflectivity moderated the relationship between self-esteem and quality of life. This relationship was such that at higher levels of self-reflectivity, low self-esteem was associated with poorer quality of life across several domains. However, at lower levels of self-reflectivity, relationships between self-esteem and quality of life were not significant. Similarly, self-reflectivity moderated the relationship between depressive symptoms and quality of life such that when self-reflectivity was high, stronger depressive symptoms were associated with poorer quality of life across several domains, but these relationships were not significant at lower levels of self-reflectivity. Importantly, moderations were significant for the anorexia group only; these patterns of relationships were not found in the bulimia group. When examining mastery as a moderator, opposite patterns were revealed. As expected, mastery significantly moderated the relationship between self-esteem and quality of life across both eating disorder groups. This relationship was such that at lower levels of mastery, low self-esteem was associated with poorer quality of life across several domains. However, these relationships were not significant at higher levels of mastery. Similarly, in the bulimia group, mastery moderated the relationship between depressive symptoms and quality of life such that higher depressive symptoms were significantly associated with lower quality of life, but only when mastery was low. These results suggest that metacognitive self-reflectivity and mastery have contrasting moderating effects and that these relationships differ between anorexia and bulimia.
These results are consistent with a growing body of work highlighting the importance of metacognition in eating disorders [16] and adds to recent work examining these constructs within the integrated model of metacognition [18]. Further, these findings extend work suggesting that impairments in the ability to think about oneself and others are transdiagnostic phenomena that have important relationships to outcomes [2, 10, 34]. Importantly, though metacognitive self-reflectivity and metacognitive mastery were not consistently associated at a bivariate level with self-esteem, depressive symptoms, or quality of life across the diagnostic groups, both self-reflectivity and mastery played a significant modifying role in the inter-relations among these variables. This is consistent with past work highlighting the role of self-reflectivity and mastery as moderating variables in other populations [22, 24] and furthers the idea that one’s ability to notice, differentiate, interpret, and integrate internal mental states and to understand and respond effectively to psychosocial challenges may alter how one is impacted by other important psychological experiences; i.e., the framework wherein one experiences and understands internal mental states impacts how those mental states have downstream effects on outcomes and other variables. This is an important insight and suggests future work should more closely consider metacognitive abilities when determining the differential impacts of psychological variables across a population.
Consistently, participants with anorexia showed significant relationships between self-esteem, depressive symptoms, and aspects of quality of life when self-reflectivity was high, while non-significant relationships between these variables were exhibited when self-reflectivity was low. Johnson-Neyman values indicated that, in large part, these transitions in significance occurred at scores of approximately 3 on self-reflectivity. At a level of a 3 (on a scale ranging from 0 to 9), participants are able to identify and distinguish between different cognitive operations (e.g., a thought, a wish, a memory), but not necessarily between emotional states or experiences [25]. Importantly, the abilities to recognize changes in mental states over time, incorporate thoughts and emotions into narratives, and integrate internal mental experiences meaningfully into one’s life narrative occur at considerably higher levels of self-reflectivity (scores 5–9), suggesting that many participants across both eating disorder samples, given the mean scores, were limited in their ability for self-reflection past acknowledgement of differing cognitive and emotional mental states.
In contrast, across both eating disorders groups, significant relationships between self-esteem, depressive symptoms, and aspects of quality of life appeared to exist when mastery was low, while at higher levels of mastery, non-significant relationships between these variables were displayed. Johnson-Neyman values indicated that these changes in significance occurred at scores of approximately 3 or lower on mastery. At a level of 3 and below on mastery, participants may be unable to identify and describe psychological distress and challenges or, if they are able to identify a psychologically distressful situation, they may be unable to respond to these challenges in a meaningful way [25]. The ability to respond to psychological challenges through behavioral inhibition, cognitive restructuring, and integration of metacognitive knowledge about themselves and others occurs at much higher levels of mastery (scores of 5–9). Like the findings for self-reflectivity, given the mean mastery scores across the sample, many of our participants proved limited in their metacognitive abilities beyond the ability to identify and describe distress.
Findings from the current study suggest that lower levels of self-reflectivity may have a protective value in anorexia, while higher levels of mastery may also possess protective value in both bulimia and anorexia. As described, the link between self-esteem, depressive symptoms, and quality of life was non-significant for those with anorexia when self-reflectivity was low. Thus, lower levels of self-reflectivity may buffer the negative impacts of low self-esteem and depressive symptoms on quality of life. Having higher self-reflectivity likely helps a person to better integrate their internal experiences, allowing them to experience the expected negative impacts of low self-esteem and depressive symptoms (i.e., poorer quality of life), while also allowing them to better access these experiences. Better awareness of and access to these experiences also opens the door to possible areas of intervention. For some, it may be beneficial to develop self-reflectivity during treatment, with monitoring and support to help navigate any potential impact on outcomes that may arise as self-reflective skills develop. While it may be protective to some extent, it is also important to note that those with lower self-reflectivity may be unable to enjoy the benefits that higher self-esteem or lower depressive symptoms can have on their quality of life. Thus, it is possible that self-reflectivity interventions may promote better quality of life outcomes when paired with interventions targeting self-esteem and depressive symptoms, though more research in this area is needed. Of note, it is possible that our findings simply reflect a lack of statistical significance. This may be related in part to our limited sample size in the moderation analyses. Further, many participants in our study had relatively low levels of self-reflectivity. Replicating this work in larger samples with a broader range of self-reflective capacity is needed to better understand these relationships.
Oppositely, higher levels of mastery may also have a protective value. Across groups, relationships between self-esteem, depressive symptoms, and quality of life were non-significant when mastery was high, suggesting that higher levels of mastery may protect against the negative impact of low self-esteem and depressive symptoms on quality of life that were observed when mastery was low. Higher levels of mastery may allow persons to better make sense of, tolerate, and respond to the distress associated with low self-esteem and depressive symptoms, resulting in a better quality of life. These results suggest that for those with eating disorders, it may be beneficial to develop metacognitive mastery skills in order to reduce the negative impact on quality of life in these groups. Of note, these moderating relationships were consistently present for those with bulimia across several quality-of-life domains; however, only one model in the anorexia group proved significant, indicating that lower self-esteem was associated with lower quality of life in the domain of social relationships. Thus, it appears that mastery may similarly affect both anorexia and bulimia. But further research is needed to investigate this.
While our results highlight metacognitive self-reflectivity and mastery as important moderating variables, they also highlight the fact that these findings are not consistent across eating disorders. Indeed, our results suggest a unique relationship with self-reflectivity in anorexia that was not present in bulimia, such that moderation was present for both self-esteem and depressive symptoms across multiple aspects of quality of life. Our results also suggest a unique relationship with mastery in bulimia that was present for both self-esteem and depressive symptoms across multiple aspects of quality of life which were not consistently observed in anorexia. There are several possible explanations for these differences between anorexia and bulimia. One possibility may be related to differences in symptomology. For example, recent work has determined that metacognition is linked to multiple forms of general psychopathology in bulimia; however, in anorexia, metacognition seems uniquely linked to disordered eating behaviors, and this group demonstrates greater impairments in metacognition [18]. Additionally, the level of insight may contribute to the differences between anorexia and bulimia. People with anorexia can experience significantly impaired insight [35, 36], which may include the inability to acknowledge their illness and symptoms. Lack of insight in anorexia has notable clinical implications, including treatment avoidance, poor treatment discipline, and assessment difficulties [37, 38]. Although we did not measure insight in this study, it is possible that self-reflectivity is related to insight in anorexia, and that both may influence the ability to acknowledge and reflect upon internal experiences such as self-esteem and depressive symptoms in a way that is unique to this population. This idea is consistent with some past work using a different model of metacognition, which found a relationship between metacognition and insight in anorexia [35]. Future work should investigate this issue.
There are several important limitations to consider. First, all of the participants in the sample identified as female, which limits the generalizability of these findings to people who identify with other genders. Additionally, the sample sizes for each diagnostic group were modest, which is important to take into account when interpreting the findings of the current study. In particular, the limited sample size in the moderation analyses may have an influence on the non-significant relationships between self-esteem, depressive symptoms, and quality of life at varying levels of self-reflectivity and mastery. Replication of this work with larger sample sizes is warranted and may further inform our understanding of the moderating relationships observed here. In the current study, we did not include a healthy control group for comparison. Further, we only focused on relationships between self-esteem, depressive symptoms, and quality of life. Deficits in interpersonal skills, social cognitive impairment, and personality traits have been implicated in eating disorders and are thought to contribute to poor outcomes [2, 39]. These relationships may also be influenced by metacognition. This is a possible avenue for future work to explore. Additionally, other variables may help to explain these relationships between metacognition, self-esteem, depressive symptoms, and quality of life. For example, neurocognitive functioning and egosyntonicity, both implicated in eating disorders [40, 41], may have an impact on the link between metacognition, self-esteem, depressive symptoms, and quality of life in this population. These variables were not assessed in this study, but future work that incorporates these variables may further inform our understanding of these relationships and have clinical implications. In addition, the current study focused on two specific domains of metacognition: self-reflectivity and mastery. Decentration and awareness of the minds of others, both additional domains within the integrated model of metacognition, should be investigated in future work. Lastly, all the data collected in the current study were done so at a single timepoint. Thus, conclusions regarding causality or how these variables may interact or change over time cannot be drawn. Further longitudinal research is needed to further examine the complexity of these relationships.
With replication, results from this study may have clinical implications for people with eating disorders. First, given the differing relationships between self-esteem, depressive symptoms, and quality of life at varying levels of self-reflectivity and mastery, metacognition should be assessed and taken into consideration in treatment planning and intervention choices. For people with anorexia, specifically, interventions targeting self-esteem or depressive symptoms may be less likely to positively affect quality of life aspects when self-reflectivity is low. Additionally, interventions focused on metacognitive ability, including Metacognitive Reflection and Insight Therapy and Metacognitive Interpersonal Therapy, could be modified for use in eating disorders. Metacognitive Reflection and Insight Therapy has been successfully adapted for use with people with psychosis across different cultures [42–45], while Metacognitive Interpersonal Therapy has been adapted for use in personality disorders [42, 46]. Either intervention could be adapted to offer improvements and improve the quality of life of people with anorexia or bulimia.
CONCLUSION
To our knowledge, this study is the first to explore metacognitive self-reflectivity and mastery as moderators in the relationship between self-esteem, depressive symptoms, and quality of life in eating disorders. The results suggest that these different metacognitive abilities have paradoxical relationships with these variables that differ between anorexia and bulimia. Specifically, the results indicate that self-reflectivity has an impact on the relationship between self-esteem, depressive symptoms, and quality of life such that when self-reflectivity is high, lower self-esteem and higher depressive symptoms are associated with a lower quality of life. In this study, these relationships existed only for those with anorexia. Oppositely, across both groups, mastery moderated the relationships between self-esteem, depressive symptoms, and quality of life such that lower self-esteem and higher depressive symptoms were associated with a lower quality of life only when mastery was low. Further work should continue to explore the complex role of self-reflectivity and mastery in eating disorders. A comprehensive understanding of these relationships is necessary to inform clinical interventions.