INTRODUCTION
Anorexia nervosa (AN) is a mental disorder that, according to the definition of the International Classification of Diseases, 11th revision (ICD-11), is characterised by a significant decrease in body weight (body mass index (BMI) <18.5 kg/m2), which is not due to the unavailability of food or another medical condition. Such conditions include: persistent restrictive eating, usually associated with a pronounced fear of weight gain; excessive concerns about weight and shape, manifested in overestimation of the importance of low body weight or incorrect perception of low body weight as normal or even excessive [1]. Thus, according to the modern definition of AN, low BMI and body image disturbance are among the key features of AN with BMI possibly being regarded as a key integral indicator characterising the clinical severity of AN [1] and body image disturbance as a key psychological component that determines the progression of the disorder [2].
Although eating disorders (ED), in particular AN, are associated with many psychological factors, for example low self-esteem and emotional dysregulation [3], one of the most important psychological factors associated with ED is perfectionism [4–6]. According to the classical transdiagnostic cognitive-behavioural model of ED by Fairburn et al. [4], perfectionism is one of the four key cognitive-behavioural mechanisms underlying ED, in particular AN. Specifically, it causes strict adherence to unrealistic standards of eating, weight, appearance, and exercise.
Later research confirms this concept [5–6]. In particular, the results of a meta-analysis by Dahlenburg et al. showed a significantly higher level of perfectionism in patients with AN compared to patients with other mental disorders and participants without diagnosed disorders [7]. In particular, when distinguishing “adaptive” perfectionism (regarded as the normal, “healthy” variant) and “maladaptive” perfectionism (the “pathological” variant), the authors identified a significant association of AN with higher rates of both maladaptive and adaptive perfectionism compared to participants without diagnosed disorders.
There are a number of research papers demonstrating the association of perfectionism with body image dissatisfaction in people without diagnosed mental disorders [8–10]. However, we did not find published works that focused on the evaluation of perfectionism linked with body image disturbance in patients with AN.
Some studies have shown association of BMI and perfectionism in adults without diagnosed mental disorders. In particular, a study by Ekici et al., 2024 [11], showed that BMI was a significant factor associated with the level of perfectionism which was evaluated using the Frost Multidimensional Perfectionism Scale (FMPS). This was based on the construction of a linear regression model, although it did not directly correlate with BMI. In an earlier study by Bernabéu-Brotóns and Marchena-Giráldez, 2022 [12], the level of perfectionism assessed using the Multidimensional Perfectionism Scale (MPS) was negatively correlated with BMI. A comparable negative correlation was also found in a Halmi et al., 2000, conducted on a sample of women with AN [13]. On the contrary, in a study Morgan-Lewis et al., 2019 [14], conducted on a sample of children and adolescents with ED, most of whom were patients with AN, BMI was positively correlated with the level of perfectionism. However, it is worth noting that this parameter in this study was assessed using the Eating Disorders Inventory-2 Perfectionism scale (EDI-P). Thus, although the existing literature data suggest an association between BMI and perfectionism, including in AN, the direction of this association remains unclear and may depend, among other things, on the characteristics of psychometric tools used for assessing perfectionism and on the diagnostic composition of the sample.
However, the very association of perfectionism and clinical indicators (in the case of AN, BMI and body image disturbance) can also be mediated by the influence of other psychological constructs of a higher order. In particular, studies have included demonstrations of the following: the moderating effects of self-efficacy [15], the persistence on the association of perfectionism and the severity of depressive symptoms [16], self-esteem on the association of perfectionism and symptoms of avoidant/restrictive food intake disorder [17], self-compassion on the association of perfectionism and anger, aggression, and hostility [18]. These aforementioned factors have demonstrated that their moderating effect are associated with metacognition [19–22].
Metacognition is a process of thinking about one’s own thoughts, controlling and regulating them, which may include attitudes to habitual thought processes, tracking mistakes, and forming a sense of the integrity of the individual, both with regard to oneself and others [23]. Previous studies have demonstrated the association of a number of metacognitive features in patients with AN, in particular negative beliefs about anxiety and beliefs about the need to control one’s own thoughts [24]. In our previous study, we identified a moderating effect of some components of metacognition, namely Self-reflectivity and Mastery (the ability to comprehend psychosocial difficulties and subsequently apply the knowledge about oneself and others obtained during metacognitive processes to choose the most effective response to them), on the association of depressive symptoms and assessment of quality of life in patients with ED [25]. In a later study by Palmeri et al. an association between the level of perfectionism and a number of metacognitive features, (in particular positive beliefs about anxiety and beliefs about the need to control one’s own thoughts), was also found in patients with ED [26].
Thus, the features of metacognition are associated with ED including AN, on the one hand, and on the other hand, with differences in the levels of perfectionism. In addition, one can assume that metacognitive features can be factors that moderate the association of perfectionism with the clinical aspects of AN: BMI and one’s body image. However, we did not find any published works on the moderating effect of metacognition on the association of perfectionism and clinical characteristics of AN. Therefore, the purpose of this study was to assess the moderating effect of metacognition on the association between perfectionism BMI and body image in patients with AN.
METHODS
Study design
A cross-sectional study was conducted.
Setting
This study included patients admitted to the Clinic for Eating Disorders of the Mental-health clinic No. 1 named after N.A. Alexeev (Moscow) from April 2023 to December 2024.
Participants
The study included all patients with a diagnosis of AN (F50.0 according to the ICD-10) admitted to the Clinic for Eating Disorders (inpatient hospital), who gave voluntary informed consent to participate in the study.
Non-inclusion criteria were hospitalisation for less than seven days and refusal to participate in the study.
Variables
BMI and body image disturbance were used as markers to assess the severity of AN.
Perfectionism was considered to be an etiological factor of AN, a stable fundamental personality trait of patients that contributes to the development and perpetuation of AN.
The level of metacognition was used as an indicator of the patient’s cognitive ability to integratively assess the surrounding world and themselves in it, i.e., perception of oneself and others, the development of adaptive behavioural strategies, and the ability to change behaviour depending on changing circumstances and external conditions.
Measurement
The examination was carried out during the first 7 days of inpatient treatment.
The diagnosis of AN was made using the clinical and psychopathological method in accordance with the ICD-10 criteria. BMI was calculated using the formula BMI=weight (kg)/height2 (m).
Body image perception was assessed using the Body Image Questionnaire (BIQ) [27]. This is a self-assessment questionnaire designed specifically to assess body image disturbance in patients with ED. It includes 16 statements assessing body satisfaction, emotional judgment of one’s appearance, behavioural strategies related to the body, and comparing oneself to other people. Each statement was rated by patients on a four-point scale (0 — “never”, 1 — “sometimes”, 2 — “often”, 3 — “always”). Higher values reflect a negative body image, a tendency to avoid social contact due to appearance, and intense comparison between oneself and others. A score of 13 and above indicates a pronounced dissatisfaction with one’s own body (sensitivity — 0.75 and specificity — 0.74). The maximum score on the scale is 48.
Perfectionism was assessed using the MPS, developed by Hewitt and Flett [28] as adapted by Gracheva [29]. This includes 45 statements split into three subscales: 1) “Self-oriented perfectionism” (striving to meet ideal personal standards), where the maximum score is 81; 2) “Others-oriented perfectionism” (excessive demands on others), where the maximum score is 51; and 3) “Socially prescribed perfectionism” (perception of society’s pressure to comply with ideals), where the maximum score is 75. MPS is a self-assessment questionnaire. The answers to the questions were recorded on a 7-point Likert scale (from “strongly disagree” to “strongly agree”). The total score for each subscale is calculated by summing the responses to the relevant items, where higher values indicate the magnitude of each of the three types of perfectionism. The integral indicator of perfectionism — the total score on all items of the scale (where the maximum is 221 points) — is also taken into account. The normative values of the integral indicator of perfectionism for the Russian population lie in the range from 160 to 204 points.
To assess the level of metacognition of patients, an abbreviated scale of metacognition (Metacognition Assessment Scale-Abbreviated, MAS-A) [30] was used; it consists of four subscales: “Self-reflectivity”, “Understanding the other’s mind”, “Decentration”, and “Mastery”. To assess metacognition, patients underwent a semi-structured Indiana Psychiatric Illness Interview (IPII) [31], during which patients described their lives and understanding of mental illness. Based on the information received, the researcher scored the patients on each subscale according to the MAS-A instruction. Scores range from 0 to 9 for the “Self-reflectivity” and “Mastery” subscales, 0 to 7 for the “Understanding the other’s mind”, and 0 to 3 for the “Decentration” subscale. In these, higher scores reflect a greater magnitude of the assessed abilities. The study used Russian-language versions of IPII and MAS-A previously used to assess the level of metacognitive abilities in patients of a Russian sample [25].
The metacognition study was conducted by medical psychologists of the Mental-health clinic No. 1 named after N.A. Alexeev, who were trained to use the scale and interpret the examination results.
Study size
A preliminary calculation of the sample size was not carried out, however, at least 100 patients were planned to be included in the study.
Bias
The study was planned, hypothesised, and conceptualised by researchers not involved in the patient examination, and the researchers involved in the patient examination were not informed about the study hypotheses. This eliminated the possibility of distorting the results of scaling to fit the hypothesis and formulating research hypotheses based on the results of patient examination. Statistical data processing was carried out by a researcher who was not involved in the collection of material, nor planning the study, nor formulating the hypothesis. Therefore it excluded the possibility of distortion of the results of data processing to fit the study hypotheses.
Statistical analysis
Statistical data processing was carried out using IBM SPSS Statistics v. 27.0 (IBM Corp., USA) with the PROCESS macro for the Johnson-Neyman procedure [32]. During the verification of the distribution of quantitative variables for normality using the Shapiro-Wilk test, the distribution of most of the variables (with the exception of BMI and MPS scores) was found to be non-normal, and therefore non-parametric statistical criteria were used in the further analysis. Correlations between the studied variables were evaluated using the Spearman correlation test. To assess the moderating effect of metacognition on the association of perfectionism with BMI and BIQ scores, multiple linear regression models were constructed with the inclusion of scores for each of the MAS-A and MPS subscales, as well as the interaction between these factors. Models with overall significance (p-value for F-test) <0.01 were selected for further interpretation. The influence of factors and their interaction was considered significant at p<0.01. The threshold value of the moderating factor (MAS-A subscale), at which the significance of the association changed, was assessed using the Johnson-Neyman procedure (p<0.05). To visualise the interaction of factors, graphs of the dependence of BMI or BIQ scores on perfectionism indicators at different levels of metacognition indicators (3 levels: the 16th, 50th and 84th percentiles) were constructed.
Ethical considerations
The study was approved by the local ethics committee of the Mental-health clinic No. 1 named after N.A. Alexeev (Report No. 2 dated March 9, 2023). All patients signed a voluntary informed consent form to participate in the study.
RESULTS
Participants
The study sample consisted of 130 patients diagnosed with AN who were admitted to the Clinic for Eating Disorders from April 2023 to December 2024 and met the inclusion criteria of the study. The majority of participants (n=125, 96.2%) were female. The median age was Me (Q1; Q3)=22 (19; 26) years.
Assessment of the scale and questionnaire results is presented in Table 1.
Table 1. Indicators of perfectionism, metacognition, and body image disturbance in the sample
|
Indicator |
Me (Q1; Q3) |
|
BMI kg/m2 |
14.7 (13.15; 16.4) |
|
BIQ |
19 (10; 28) |
|
MAS-A Self-reflectivity (0–9) Understanding the other’s mind (0–7) Mastery (0–9) Decentration (0–3) |
3 (2; 5) 3 (2; 4) 2 (1; 3) 1 (1; 2) |
|
MPS Self-oriented perfectionism (max. 81) Others-oriented perfectionism (max 51) Socially prescribed perfectionism (max 75) Integral scale (normal range 160–204) |
69 (53; 81) 45.5 (35.75; 57.25) 52.5 (41.75; 64) 166 (135.5; 194) |
Note: BIQ — Body Image Questionnaire; BMI — Body Mass Index; MAS-A — Metacognition Assessment Scale-Abbreviated; Me — median; MPS — Multidimensional Perfectionism Scale.
Correlations between perfectionism, body image disturbance, metacognition, and BMI
When constructing the correlation matrix, significant positive correlations of all subscales of perfectionism with a negative attitude to one’s own body on the BIQ scale were revealed (Table 2). Significant correlations of moderate strength were noted with Others-oriented perfectionism and Socially prescribed perfectionism (ρ=0.545 and ρ=0.478, respectively). The level of “Self-reflectivity” and “Understanding the other’s mind” on the MAS-A scale was slightly negatively correlated with a “Negative attitude towards one’s own body” on the BIQ scale. “Mastery” and “Understanding the other’s mind” MAS-A subscale scores were positively correlated with BMI, however, the correlation strength was weak (ρ=0.249 and ρ=0.178, respectively).
Table 2. Correlations between perfectionism, body image disturbance, metacognition, and BMI
|
Indicators |
BMI |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
|
1. BIQ |
0.04 |
− |
− |
− |
− |
− |
− |
− |
− |
|
2. MAS-A-S |
0.127 |
−0.213* |
− |
− |
− |
− |
− |
− |
− |
|
3. MAS-A-O |
0.178* |
−0.197* |
0.482** |
− |
− |
− |
− |
− |
− |
|
4. MAS-A-M |
0.249** |
−0.168 |
0.515** |
0.728** |
− |
− |
− |
− |
− |
|
5. MAS-A-D |
−0.033 |
−0.145 |
0.329** |
0.381** |
0.397** |
− |
− |
− |
− |
|
6. MPS-SOP |
−0.069 |
0.268** |
−0.022 |
−0.029 |
−0.121 |
0.125 |
− |
− |
− |
|
7. MPS-OOP |
−0.045 |
0.545** |
−0.043 |
−0.125 |
−0.183** |
−0.055 |
0.510** |
− |
− |
|
8. MPS-SPP |
−0.030 |
0.478** |
0.037 |
−0.023 |
−0.050 |
0.081 |
0.804** |
0.762** |
− |
|
9. MPS-IS |
−0.030 |
0.478** |
0.037 |
−0.023 |
−0.050 |
0.081 |
0.804** |
0.762** |
0.845** |
Note: The table shows Spearman correlation coefficients. * p<0.05; ** p<0.01. BIQ — Body Image Questionnaire; BMI — Body Mass Index; MAS-A-D — MAS-A-Decentration; MAS-A-O — MAS-A-Understanding the Other’s Mind; MAS-A-M — MAS-A-Mastery; MAS-A-S — MAS-A-Self-Reflectivity; MPS-IS — Integral Scale; MPS-OOP — MPS-Others-Oriented Perfectionism; MPS-SOP — MPS-Self-Oriented Perfectionism; MPS-SPP — MPS-Socially Prescribed Perfectionism.
Moderating effect of metacognition on the interaction of perfectionism with body image disturbance and BMI
During the construction of multiple linear regression models, a significant influence of the level of perfectionism on BMI was revealed when Mastery was included in the model as a moderating factor. Here, a significant influence of the level of perfectionism on the BIQ score under the influence of self-reflectivity and mastery as moderating factors was observed (Table 3, Figure 1 and Figure 2). The results of constructing multiple linear regression models with a level of statistical significance from 0.01 to 0.05 are presented in Table S1 in the Supplementary.
Table 3. Influence of perfectionism and metacognition indicators and their interactions on BMI and body image
|
Variable |
Coefficient B [95% CI] |
Standard error |
t |
p |
|
BMI (R2=0.12, F=5.259, p=0.002) |
||||
|
Constant |
17.52 [14.403; 20.638] |
1.5746 |
11.1271 |
<0.0001 |
|
MPS-Integral Scale |
−0.023 [−0.042; −0.004] |
0.0094 |
−2.4492 |
0.0158 |
|
MAS-A-M |
−1.0195 [−2.013; −0.026] |
0.5017 |
−2.0322 |
0.0444 |
|
Interaction (change R2=0.062) |
0.009 [0.003; 0.015] |
0.0031 |
2.8978 |
0.0045 |
|
BMI (R2=0.135, F=6.183, p=0.0006) |
||||
|
Constant |
17.594 [14.982; 20.206] |
1.3192 |
13.3369 |
<0.0001 |
|
MPS-OOP |
−0.086 [−0.142; −0.03] |
0.0283 |
−3.0273 |
0.003 |
|
MAS-A-M |
−0.929 [−1.753; −0.105] |
0.4161 |
−2.2328 |
0.0274 |
|
Interaction (change R2=0.08) |
0.0312 [0.013; 0.05] |
0.0094 |
3.3145 |
0.0012 |
|
BIQ (R2=0.21, F=10.778, p<0.0001) |
||||
|
Constant |
26.762 [11.839; 41.685] |
7.537 |
3.5508 |
0.0005 |
|
MPS-SOP |
−0.052 [−0.274; 0.171] |
0.1123 |
−0.4602 |
0.6462 |
|
MAS-A-S |
−6.372 [−10.219; −2.525] |
1.9429 |
−3.2796 |
0.0014 |
|
Interaction (change R2=0.049) |
0.078 [0.021; 0.135] |
0.0285 |
2.7311 |
0.0073 |
Note: BIQ — Body Image Questionnaire; BMI — Body Mass Index; CI — confidence interval; MAS-A — Metacognition Assessment Scale-Abbreviated; MAS-A-M — MAS-A-Mastery; MAS-A-S — MAS-A-Self-Reflectivity; MPS — Multidimensional Perfectionism Scale; MPS-OOP — MPS-Others-Oriented Perfectionism; MPS-SOP — MPS-Self-Oriented Perfectionism.
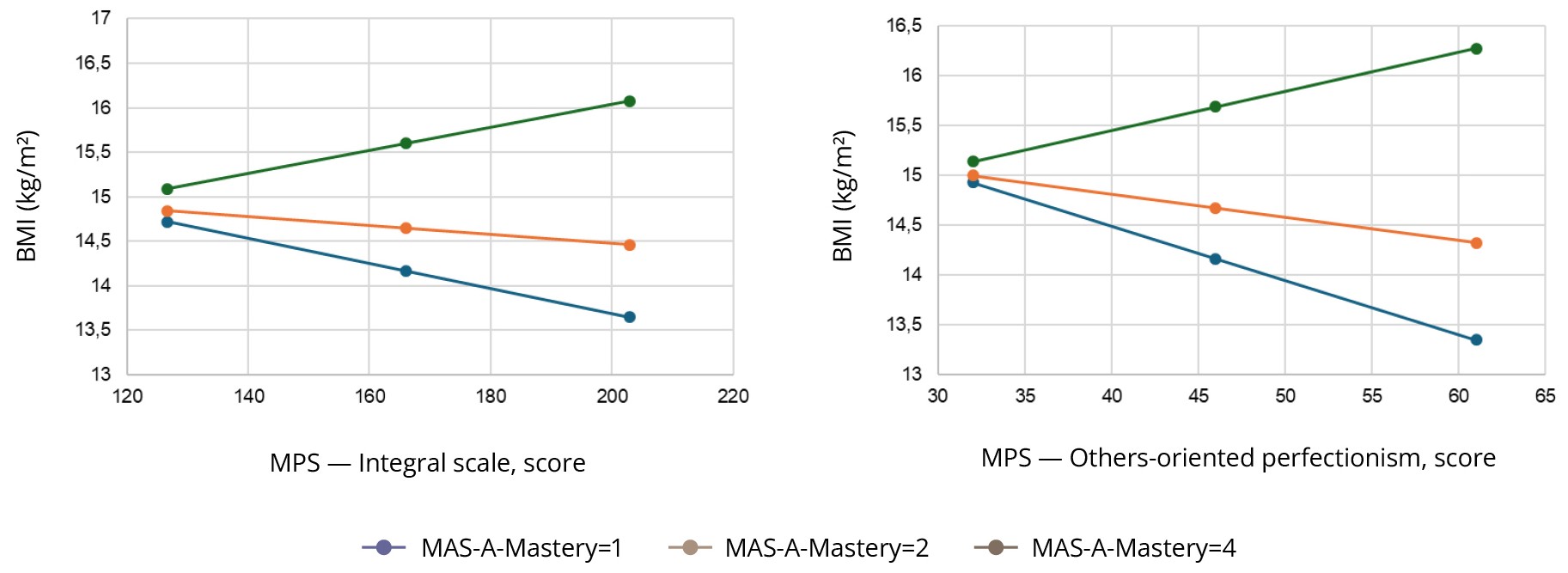
Using the Johnson-Neyman technique, a significant association of the integral scale of perfectionism and BMI was noted at Mastery values below 1.076 (30.9% of the sample) and above 3.956 (16.2% of the sample). Similar results were obtained during the construction of the model with the inclusion of the factors of Mastery and Others-oriented perfectionism: a significant association of Others-oriented perfectionism with BMI was noted at Mastery values below 1.748 (30.9% of the sample) and above 3.8312 (16.2% of the sample). An increase in the level of perfectionism is associated with a decrease in BMI at low MAS-A-Mastery (1 or less), but at higher values (4 or more) it is associated with an increase in BMI (Figure 1, Tables S2 and S3 in the Supplementary).
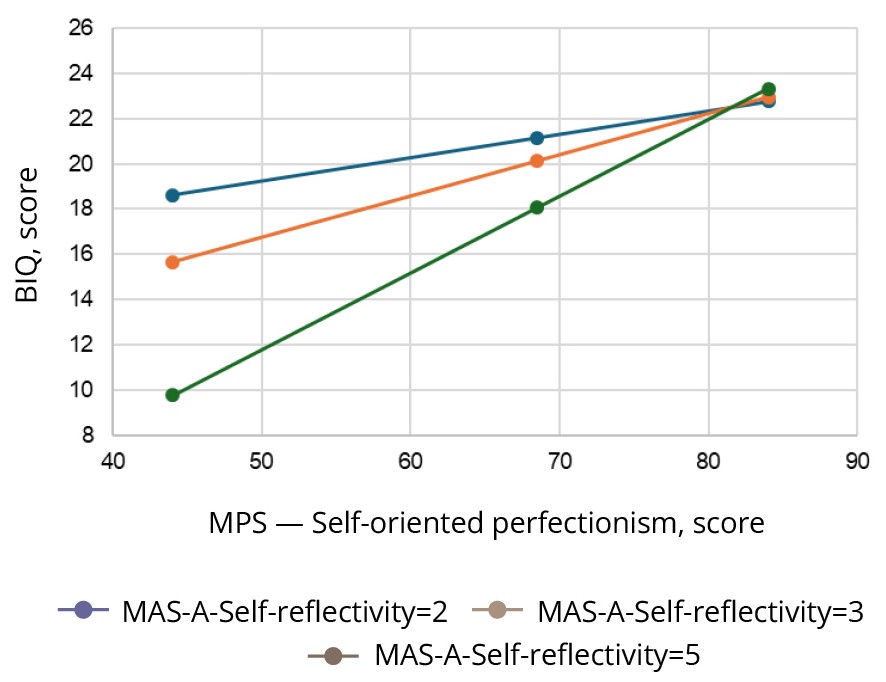
When constructing a model with the inclusion of Self-oriented perfectionism, a significant association of Self-oriented perfectionism with the BIQ score was noted at Self-reflectivity values >2.2316 (65.3% of the sample) (Figure 2, Table S4 in the Supplementary). This model demonstrates that at a high level of Self-reflectivity and a low level of perfectionism there is a lower intensity of body image disturbance, but with an increase in the level of perfectionism on these subscales the intensity of negative body image increases at Self-reflectivity scores of 2 or higher.
DISCUSSION
Metacognition had a moderating effect on the association between perfectionism and BMI and body image disturbance, while the direction of this association depended on the magnitude of the individual components of metacognition. At Mastery scores of ≥4, higher Others-oriented perfectionism scores were associated with an increase in BMI, and at Mastery scores of ≤1, a higher level of Others-oriented perfectionism was associated with lower BMI. Even with minimally pronounced Self-reflectivity (≥2), the negative effect of Self-oriented perfectionism on body image was evident.
At the same time, no significant correlation was found between BMI and perfectionism, which contrasts with some studies where significant associations were identified [11–14]. Disturbance of body image positively correlated with all manifestations of perfectionism, which is consistent with data from previous studies in non-clinical samples [8–10].
It has been shown that Others-oriented perfectionism can have the opposite effect on BMI depending on the patient’s ability to respond effectively to the situation (Mastery). It can become “malignant” and contribute to a decrease in BMI in patients with low adaptation skills, while contributing to an increase in BMI in patients with good adaptation skills. This observation can be explained by the patient’s ability to direct their attention away from their own imperfections to the imperfections of the people around them, which in turn lessens fixation on their own weight.
We can put forward several hypotheses to explain this connection. First, when others do not meet the perfectionist standards of appearance or behaviour, this causes frustration and anxiety in patients with low Mastery as they perceive this as a lack of support for their strict beliefs, which increases self-criticism and restrictive eating, reducing BMI. For example, a patient may experience stress if their significant others do not support their dietary practices, leading to increased control over the body as a way to compensate. Second, perceptions of others’ imperfections may reflect their own perfectionist beliefs about themselves, increasing anxiety as patients perceive others as weak, unable to control their weight and diet, and a demonstration of the need to stay fit. This process can strengthen fixation on control of their appearance, which also contributes to a decrease in BMI. On the contrary, at high levels of Mastery mentalization allows patients to be more flexible about expectations from others, re-evaluating them as unrealistic, which synchronizes with the transformation of their own perfectionist standards. High adaptive skills lessen the role of perfectionism as a key life management strategy, allowing patients to use alternative coping strategies such as setting realistic goals or managing emotions, which reduces the need for weight control and promotes healthier eating behaviours, and increasing BMI [9, 33]. These findings are consistent with studies emphasising the role of metacognitive processes in improving psychosocial functioning and emotional regulation, and confirm the potentially adaptive role of perfectionism in the presence of effective regulatory mechanisms [34].
At the same time, under the influence of a minimum level of Self-reflectivity, Self-oriented perfectionism leads to body image disturbance.
We suggest that this type of perfectionism encourages patients with AN to set unrealistic standards for their appearance, which increases Self-criticism and body dissatisfaction. At a minimal level of Self-reflectivity, patients are able to be aware of their shortcomings, but do not have sufficient metacognition skills to critically re-evaluate these beliefs or reduce their emotional impact. This leads to fixation on the negative aspects of the body image, which is confirmed by high BIQ scores. Our data are consistent with current research. Studies of metacognitive processes confirm that limited Self-reflectivity, especially in the form of rumination, contributes to fixation on the negative aspects of body image and intensifies the symptoms of AN [35, 36]. In addition, research emphasises that Self-oriented perfectionism increases self-criticism and body dissatisfaction, which is manifested in a pronounced preoccupation with body image [37].
Overall, patients in the study showed low levels of metacognition across all MAS-A subscales, limiting their ability to cope with the challenges of recovering from AN. Low Self-reflectivity, Understanding the other’s mind, Decentration, and low Mastery can hinder effective re-evaluation of perfectionist ideas and social expectations, as well as emotional management, which exacerbates symptoms of AN, such as body image disturbance and restrictive eating. In addition, perfectionism indicators in our sample were in the average range, which differs from studies that found a stronger association of perfectionism with AN symptoms, BMI, and body perception when perfectionism scores in the sample were high [6].
The main limitation of the study was the use of self-assessment questionnaires to evaluate the level of perfectionism and body image disturbance. Although both questionnaires were tested in the Russian-speaking population, the use of self-assessment questionnaires in patients with AN, especially in cases of acute manifestations of the disorder, may not show reliable results due to the tendency of patients to downplay the severity of their symptoms. In particular, lower rates of perfectionism in our study compared to other AN studies may be associated with additional factors affecting the quality of filling out self-assessment questionnaires, such as physical and psychological exhaustion of patients, low motivation to participate in the study, and a tendency to conceal the clinical picture [38].
Our findings demonstrate the links between perfectionism, metacognition, body image disturbance, and BMI in patients with AN and open up a number of questions requiring further investigation.
One key issue is establishing the causal relationship between perfectionism, body image disturbance, and BMI. It is unclear whether perfectionism is the cause of body image disturbance that lead to restrictive eating and decreased BMI, or whether low BMI associated with malnutrition reinforces perfectionist tendencies and body image disturbance through neurobiological and psychological mechanisms. For example, perfectionism can motivate strict dietary practices, thus reducing BMI, but malnutrition, as shown in studies, increases cognitive distortions, including preoccupation with the body, which in turn reinforces perfectionism [39]. Perfectionism is closely linked with anxiety, depression, and low self-esteem, which are comorbid symptoms of AN and can modulate the interaction between BMI, perfectionism, and body image [25]. It is unclear whether perfectionism itself is an independent predictor of body image disturbance and BMI disorders, or its effect is mediated by emotional factors. For example, anxiety can heighten the perception of social pressure associated with Socially prescribed perfectionism, which increases preoccupation with the body, while depression can exacerbate the rumination associated with Self-reflectivity.
CONCLUSION
The association between perfectionism and body image disturbance and BMI in patients with AN depends on the magnitude of Self-reflectivity and the ability to develop adaptive strategies for coping and regulating behaviour (Mastery). The obtained data indicate the necessity of incorporating psychotherapy aimed at the development of metacognition in patients with AN. The target of this psychotherapy may be Self- and Others-oriented perfectionism as a factor that affects key clinical indicators in AN — body image disturbance and BMI — depending on the magnitude of Self-reflectivity and Mastery.