Introduction
Attention deficit hyperactivity disorder (ADHD) is one of the most common behavioral disorders that are diagnosed at different stages of human ontogenesis. The estimated worldwide prevalence of ADHD is 7.2% [Thomas, 2015]. The interest in understanding the causes and mechanisms of this clinical entity is increasing due to its important relationship with school academic performance [Pastor, 2008]. Clinical reports and descriptions of ADHD cases have focused on the child population [Benzing, 2017]. Some authors claim that the disorder also might depend on psychological and social factors, such as family situation, the child, and the school’s teaching methods [Glozman, 2014].
In the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) [American Psychological Association] the biomedical paradigm is strengthened by a change of emphasis on preventive psychiatry. The current aim of psychiatric nosology is the early identification of the psychopathology, in order to prescribe adequate interventions before the establishment of possible mental health problems, by introducing new diagnoses and lowering existing thresholds [Koutsoklenis, 2019]. Some authors found that ADHD is a psychiatric diagnostic entity, as a historical, cultural, and political category that fulfills certain functions [Koutsoklenis, 2019] as opposed to a simple neurobiological category. Nevertheless, in the clinical practice of most countries, the diagnosis of ADHD is used as an independent nosological entity, which causes ambiguity in terms of understanding its causes and the possibility of treatment.
However, there are no measurable biomarkers or objective tests to establish the presence or absence of ADHD as a natural disorder from the early stages of an individual’s development [Thome, 2012]. This position is supported by a meta-analysis, which found that ADHD lacks a specific etiology and there are no unique characteristics or laboratory indices to support its diagnosis. In addition, this category is based on the history of the syndrome itself, as well as observing and describing specific behaviors and symptoms [Wang, 2017].
The specific medical treatment for ADHD and its effects on children is another point of discussion in the literature. The most common treatment consists of administering psychostimulants. The effect of such treatment, considering the diversity of possible causes and absence of homogeneity, are debatable. In a recent study a group of adolescents with ADHD demonstrated poor therapeutic adherence and an indifferent attitude towards medication. However, the authors report that drugs can be useful in optimizing treatment and reducing external symptoms [Kosse, 2017].
The previous research indicates that children and adolescents with different clinical characteristics can fall under a single diagnosis and receive the same pharmacological treatment without sufficient justification. The same behavioral symptoms might be caused by a wide range of cerebral, physiological, and social reasons. For this reason, equating children from a neuropsychological and neurophysiological standpoint according to the data from the interviews based on the DSM-5 diagnostic checklist does not seem to be ideal for establishing diagnoses and treatments [Solovieva, 2017a].
This position is supported by electroencephalographic studies demonstrating that abnormal brain electrical activity in subjects with ADHD may be associated with deficit of functioning of different subcortical brain systems that support information processing and executive control processes [Machinskaya, 2014]. Different disciplines and approaches may propose their own strategies for analysis of brain mechanisms, which underline the symptoms described in cases of attention deficit.
One of such approaches is cognitive-quantitative neuropsychology. From this perspective, the authors consider that ADHD occurs due to developmental failure of the brain circuits responsible for inhibition of attention and behavioral and emotional self-regulation [3;4], as well as due to impaired executive functions and working memory [Hoogman, 2017].
Quantitative neuropsychology focuses primarily on psychometric techniques applied to diagnostic problems, to the detriment of systematic attempts to construct a working theory of the functional organization of the brain in relation to the psychological processes [Luria, 1977]. In this case, ADHD might be associated with deficits in different cognitive domains based on mistakes during the performance of subjects in psychometric tests.
Another approach is qualitative neuropsychology, proposed by Vigotsky, Luria and cultural-historical approach [Luria; Luria, 1966; Luria, 1973]. This approach considers the possibility of generalizing clinical pictures not by behavioral traits, but by the type of brain functional mechanisms (or neuropsychological factors) that underline different cognitive tasks [Thomas, 2015]. This provides a new understanding of the neuropsychological syndrome, which means the identification of common features in mistakes and the process of performance in different tasks. Such a procedure is called the psychological qualification of the deficit and allows one to find a common factor, which underlines disturbances in different functions [Luria, 1970; Mikadze, 2019].
The neuropsychological factor is a specific term used only within the cultural-historical approach might be understood as a brain functional mechanism of the brain functional system. Such an approach makes it possible to establish different levels of analysis during the neuropsychological assessment. These levels are (i) brain level, related to the functioning of specific brain mechanisms, and (ii) psychological level, related to the psychological phenomena produced by the functioning of this mechanism [Mikadze, 2019]. Functional brain mechanisms are organized into complex functional blocks of complex cortical-subcortical relationships [Ardila, 2020; Luria, 1966; Luria, 1973]. These relations are flexible, dynamic, and changeable during different periods of ontogenetic development according to types of cultural activity [Solovieva, 2019].
According to Luria’s approach, the neuropsychological investigation is based on the assumption that each psychological action is represented in the brain as a complex flexible functional system that reflects the joint functioning of groups and levels of brain zones. Each brain area has its own highly specific work, which plays the necessary role in effectively performing complex psychological activities. In case of disturbances in any brain area, the whole functional system would suffer; this suffering would be different according to each precise level of involved neuropsychological factors [Luria, 1970].
Syndromic or dynamic neuropsychological analysis has three main advantages: 1) it contributes to a greater diagnostic accuracy in terms of brain functionality, 2) allows differentiating between conditions that may be externally similar, but internally different, and 3) provides the methodological bases to create corrective methods and work pathways [Luria].
Brain functional mechanisms, detected during qualitative assessment of school children with diagnosis of attention deficit disorder in Mexico, were studied in previous studies. Qualitative neuropsychological assessment was applied to pupils between 7 and 9 years (n=20) and 9 to 12 years (n=14). Qualitative syndromic analysis of younger pupils of primary school established four neuropsychological profiles according to specific types of functional deficits, which were: 1) deficit of voluntary regulation and control, 2) low level of nonspecific brain activation, 3) deficit of spatial analysis and synthesis and 4) deficit of sequential organization of movements and actions. In older pupils, combined profiles of deficits in regulation and control and spatial analysis and synthesis were also observed, as a combination of profiles 1 and 3. Visual qualitative analysis of EEG, in each particular type of neuropsychological profile, was related to specific EEG abnormal patterns. These patterns reflected immaturity and/or suboptimal functioning of cortico-subcortical regulatory systems of the brain [Solovieva, 2016; Solovieva, 2016a]. These data underscore the absence of a single neuropsychological profile and electrophysiological pattern that underlie the attention deficit syndrome throughout the school-age years.
Adolescence is a period with less systematization of ADHD clinical data (deficit of brain functional mechanism) and treatment recommendations; however, this population also attracts the interest of investigators [Bonilla-Sánchez, 2018; Liu C.-Y, 2021; Machinskaya, 2020]. The aim of this study was to describe the neuropsychological profiles and electrophysiological patterns that underline ADHD in early adolescence, according to methodology of qualitative neuropsychological assessment, proposed by the cultural-historical approach.
Research program
Participants
The sample consisted of 20 Mexican teenagers, enrolled in a public secondary school, divided into two groups: 10 control and 10 experimental subjects (diagnosed with ADHD). Both groups exhibited similar sociodemographic characteristics, in terms of sex, age and educational level.
The inclusion criteria for the experimental group were the following: 1) the age between 12 and 15 years, 2) being a student enrolled in a public urban secondary school, 3) being previously diagnosed with attention deficit disorder with or without hyperactivity (ADD or ADHD), determined independently by a neuropediatrician, child and adolescent psychiatrist, neurologist or school psychologist, according to DMS-IV or DMS-5 criteria, and 4) exhibiting symptoms 6 months before assessment that manifested themselves in at least two environments (school, family, etc.).
The main reasons for medical and/or psychological consultation were learning problems and poor academic performance. Moreover, at the initial interview, the parents of adolescents with ADHD reported that professional care was not entirely efficient, including the pedagogical and medical strategies they had previously experienced.
As for the control group, the inclusion criteria were the following: 1) the age between 12 and 15 years, 2) being a student enrolled in the same public urban secondary school as experimental subjects, 3) absence of diagnoses of attention deficit disorder or any other neurological or psychiatric diagnosis.
All adolescents of both groups participated in the study according to the Declaration of Helsinki. Their participation was voluntary; written informed consent was obtained from the families and teachers for neuropsychological and EEG assessments. The study was approved by the local research ethics committee.
Instruments
During the study, all participants were submitted to the following procedures: a semi-structured clinical interview, qualitative neuropsychological assessment, and EEG recording. For the semi-structured interview, a flexible format was used to obtain information on the perinatal and postnatal ontogenetic development of each participant, in order to rule out alternative medical conditions other than attention deficit.
Qualitative neuropsychological assessment
Clinical neuropsychological assessment was conducted by evaluating the neuropsychological factors using tests designed for this purpose. The Brief Neuropsychological Assessment of Adults [Quintanar, 2013] represents a sensitive exploration of neuropsychological factors described in Table 1. This assessment involves different task modalities: tactile-motor, visual, verbal, and graphic (guided and independent drawing). Additionally, oral word association and oral conflict tests were used as a part of the Brief-Puebla Neuropsychological Assessment of Children protocol / ENIB-Puebla [Solovieva, 2017]. The aim of this test is to assess regulation and control in completing a motor program with verbal instructions. Table 1 represents the relation between the tasks of the protocol of neuropsychological assessment and neuropsychological factors with its specific function in psychological tasks.
Syndromic analysis
After the neuropsychological assessment, all executions were submitted to syndromic analysis, which means analysis of different mistakes and behavior of participants during the performance in the proposed tasks. A large number of symptoms should be reduced to a common reason of deficit of a specific brain mechanism or factor. This method can only be used in its entirety for qualitative analysis of the symptoms of each particular subject in order to find the factor underlying the difficulties and relate it to specific brain level [Luria, 1970]. In each adolescent, the answers obtained in the entire neuropsychological assessment protocol were analyzed in order to identify the neuropsychological profile underlying each clinical picture.
Table 1
Structure of the qualitative neuropsychological assessment protocol
|
Neuropsychological factor or brain functional mechanisms |
Function |
Tasks for assessment |
|
Brain non-specific activation |
Level of general brain tonus needed for the normal working of the cerebral cortex and stability of task execution |
— Level of stability observed throughout the subject’s execution of the assessment protocol |
|
Phonematic integration |
Differentiation of verbal sounds according to phonemic contrast in words with different meaning in each concreate language |
— Repetition of phonologically opposite pairs of words and syllables — Identification of specific phonemes — Identification of sounds (first and second) in words |
|
Kinesthetic-tactile analysis and synthesis |
Fine tactile sensitivity as well as proprioceptive precision of postures and poses; articulation of oral speech by differentiation of verbal sounds according to the mode and location of motor production |
— Reproduction and retention of finger positions with closed and opened eyes. — Reproduction of phonoarticulatory poses (inflating cheeks, blowing, tongue movements) — Repetition of syllables and sounds with articulatory close sounds |
|
Audio-verbal retention |
Ensures the stability of memory traces (volume of perception) in the audio-verbal modality |
— Reproduction, simple recall and recall after heterogeneous interference of series of words |
|
Visual retention |
Ensures the stability of memory traces (volume of perception) in the visual modality |
— Reproduction, simple recall and recall after heterogeneous interference of series of meaningless figures |
|
Spatial integration |
Guarantees the perception and adequate production of essential features and their location, metric aspects, and the spatial relationships between the elements of the situation. |
— Understanding of instructions related to orientation in the body scheme — Understanding of complex logical-grammatical sentences — Perception of numbers and letters — Copy of a complex model (house with perspective) — Free drawing of animals |
|
Sequential organization of movements and actions |
Guarantees fluent transition from one movement to another, inhibits the anterior motor link for flexible passage to the posterior motor link |
— Sequence of hand movements (execution with / without language) — Copy of a graphic sequence with changing graphic patterns |
|
Regulation, programming and control of voluntary actions |
Ensures task execution according to the objective (the instruction or the rule), the established program and its final verification |
— Observation of subject’s performance — Oral word association test — Oral conflict test |
Electroencephalogram (EEG)
The NicView System (Nicolet Biomedical Inc.) was used for EEG recording, with sampling frequencies of 250 Hz and 19 electrodes placed according to the international 10-20 system: O1, O2; P3, P4; C3, C4; T3, T4; T5, T6; F1, F2; F3, F4; F7, F8; Pz; Cz and Fz. The recording was made in a waking state and the following maneuvers performed: a) opening and closing the eyes, b) Rhythmic photo stimulation at frequencies from 8 to 12 Hz in 1-Hz steps. The duration of the period of light stimulation and the interval between stimuli were equal and amounted to 10 s c) hyperventilation (90 seconds).
Monopolar and bipolar montages were used for each recording. Monopolar montage makes it possible to assess the bilaterally synchronous EEG patterns, which reflect the suboptimal functioning of different deep brain regulatory structures. On the contrary, bipolar montage evaluates the functional states of different brain cortical areas [20;35]. EEG recording was applied to 10 adolescents from experimental and 5 from the control group.
Visual qualitative analysis of EEG
The adolescents’ brain electrical activity was analyzed using visual qualitative analysis of different abnormal EEG pattern identified in clinical EEG studies [Huges, 1994]. The original scheme was applied for qualitative analysis of EEG, assessing the EEG parameters grouped into four blocks in relation to the systemic organization of the brain [Machinskaya, 1997]. Table 2 shows EEG parameters for each functional block, variables, which might be detected on EEG for each parameter and the function of variables.
Source: Adapted from [Solovieva, 2013] and [Machinskaya, 2020].
These parameters make it possible to assess the functional state of the cerebral cortex and its relationship with age, diffuse brain electrical activity changes, functional state of the different cortical areas of each hemisphere, and subcortical regulatory systems [Solovieva, 2013].
Procedures
The initial interview was administered to the participants’ caregivers in an individual session lasting approximately 1 hour. The same neuropsychological assessment was applied to all adolescents at the Neuropsychology Service of the University Hospital of Puebla, Mexico. The sessions were held individually and lasted 90 minutes. Later, adolescents with ADHD and 5 participants of the control group were submitted to EEG recording at the Neuropsychology and Psychopedagogy Institute of Puebla, Mexico.
Data analysis
The qualitative analysis consisted of identifying the conserved and altered neuropsychological factor in each adolescent based on typical errors. In addition, the visual qualitative EEG parameters were analyzed in each recording (Table 2), forming the electroencephalographic results of the study. Next, certain group trends were established based on neuropsychological performance and EEG profiles.
Table 2
Parameters for visual qualitative analysis of the EEG
|
Parameters |
Variables |
Functions |
|
(1) Functional state of the cortical rhythmogenic mechanisms |
— Characteristics of the alpha rhythm: regularity, topography, frequency range, amplitude, alpha rhythm asymmetries. — Reaction to the functional probes (opening and closing of eyes, rhythmic photo stimulation and hyperventilation) |
— Level of cortex excitability. — Manifestation correspondence with the relevant age norm |
|
(2) General and diffuse changes of the brain functional state |
— Diffuse sharp waves of different frequency ranges (alpha, theta, delta, beta) without particular location |
— Manifestation of diffuse changes of the brain activity (Slight/ pronounced changes) |
|
(3) Local changes of the brain cortex activity |
Type, topography, asymmetries of local deviated electrical activity (LDEA), its reactions to functional probes |
— LDEA location — LDEA origin (cortical or subcortical) — LDEA character (functional, paroxysmal, pathological) — LDEA manifestation. |
|
(4) The condition of the deep brainstem and subcortical structures. |
— Type, topography, asymmetries of generalized or bilateral synchronized deviated electrical activity (BSDEA). — BSDEA reactions to functional probes |
— Deep structure level that produces changes in the EEG: caudal brain stem, mesencephalic, limbic, diencephalic (hypothalamic), frontal-thalamic, fronto-basal. — Character of EEG changes (functional, paroxysmal, pathological) |
Table 3
Types of errors in adolescents with ADHD observed in the
neuropsychological assessment tasks
and their relationship with a specific neuropsychological factor
|
Errors related to reduced arousal level |
Errors related to the deficit of kinesthetic analysis and synthesis |
Errors related to the deficit of regulation and control of activity |
|
— Slow execution of motor and verbal tasks — Latency in verbal tasks — Micrography in graphic tasks — Fluctuations in the graphic task trace — Loss of horizontality in graphic tasks |
— Incorrect articulatory movements (especially in precise tongue movements) — Inability to reproduce positions with the fingers — Sound distortion and substitution (dentoalveolar: /d/, /t/, /r/, /l/) in verbal tasks — Phonetic/phonological substitution of sounds in all verbal tasks |
— Simplifications (graphic / motor) — Disorganization of execution in graphic, verbal and motor tasks — Loss of objective in graphic and motor tasks — Impulsiveness and anticipation of graphic and motor task activities — Loss of information (without losing the objective) in verbal memory tasks — Problems in controlling/verifying graphic and verbal tasks — Semantic substitutions (determined by the phonological context) in verbal tasks — Partial loss of baseline in graphic tasks — Intrusion of elements in graphic and verbal tasks |
Results
The results of neuropsychological assessment and syndromic analysis method made it possible to identify types of errors for the 10 adolescents from the ADHD group in order to organize neuropsychological profiles. Table 3 shows three profiles found in the study according to the analysis of errors: 1) errors related to brain non-specific activation or arousal level; 2) errors related to kinesthetic analysis and synthesis; 3) error related to regulation, programming, and control of voluntary activity.
The results of the study show differences in tasks performance among adolescents with ADHD. The mistakes were related to the functional state of different brain mechanisms. The incidence of these types of errors in each case allowed to establish clinical neuropsychological profiles. Each profile corresponded to the typical difficulties and errors found during the neuropsychological assessment.
Thus, the following profiles of adolescents with ADHD were formed: 1) with the deficit of regulation and control of activity [n=5], 2) with the deficit of regulation and control and with reduced brain arousal level [n=3], 3) with the deficit of regulation and control and with deficit of kinesthetic analysis and synthesis [n=1], 4) absence of neuropsychological profile [n=1]. One adolescent from the ADHD group did not demonstrate any cognitive or regulatory difficulties during neuropsychological examination [absence of neuropsychological profile, n=1].
According to the results of the assessment of adolescents of both experimental and control groups, optimal performance was found for the following neuropsychological factors: phonematic integration, audio-verbal retention, visual retention, spatial integration, and sequential organization of movements and actions.
As expected, the control group exhibited no systematic errors related to the functioning of neuropsychological factors, that is, optimal performance in the proposed tasks during the assessment. The errors observed had no systemic effect, since they were sporadic and not repeated in the tasks of different verbal, graphic, and motor tasks.
Physiological study results (EEG)
According to the scheme of EEG structural analysis (Table 2), various electroencephalographic phenomenon, such as rhythmic oscillations of a certain frequency or individual deviating patterns, depending on their regularity, shape and topography belong to four functional classes that characterize the condition of the cerebral cortex and deep regulatory structures of the brain. Considering the objectives of the present study, we describe the EEG patterns of the experimental group compared to the control group together with the relation of these patterns to the results of neuropsychological assessment.
Analysis of EEG data of 5 adolescents of the control group found out a modulated alpha rhythm of approximately 11Hz, mean amplitude of 60-110µV, and occipito-parietal topography with right posterior temporal extension, which corresponded to the age norm. The EEG showed absence of functional changes of local, diffuse, bilateral, and/or generalized character.
The EEG data of adolescents of the experimental group showed a background rhythm compatible with the age (compared with EEG data of the control group), that is, all participants of both groups exhibited an optimal cortical rhythmogenesis and excitability level, according to the first parameter of qualitative analysis. No difference according to the second parameter (general and diffuse changes) was found between the subjects from the control and experimental group.
The differences between the participants of experimental groups and the control group were found for to the third type of EEG patterns related to local changes of the brain cortex activity and also for the fourth type related to the functional state of the deep brain regulatory structures.
Most of the deviated EEG patterns, observed in our study were related to suboptimal functioning of the brain subcortical or cortico-subcortical regulatory system (the fourth type of EEG changes according the structural EEG analysis). The EEG changes of different frequency, waveform and topography were attributed to the suboptimal condition of the different brain deep structures. The characters of these patterns and their associations with the brain structures are shown in Table 4 (for more information see [Machinskaya, 2014].
Table 4
EEG patterns reflecting suboptimal functioning of the deep brain structures
|
Brain structures |
EEG pattern |
|
Basal ganglia |
Bilateral synchronous bursts of the spindle-like β-activity (20—30 Hz) in the frontal, central, and/or anterior temporal leads |
|
Hypothalamus |
Generalized bilaterally synchronous oscillations of different frequencies, sometimes including sharp monophasic and/or biphasic spikes, alpha or beta-spindles |
|
Limbic |
Bilaterally synchronous spindle-like oscillations of 6—10 Hz (low alpha range) in the frontal and/or fronto-temporal leads |
|
Fronto-thalamic |
Bilaterally synchronous groups of theta waves (4—6 Hz) in the only frontal or in the frontal and central leads |
|
Mesencephalic |
Bilaterally synchronous groups of theta waves in the posterior and central leads |
|
Brainstem |
Generalized bilaterally synchronous groups of theta waves |
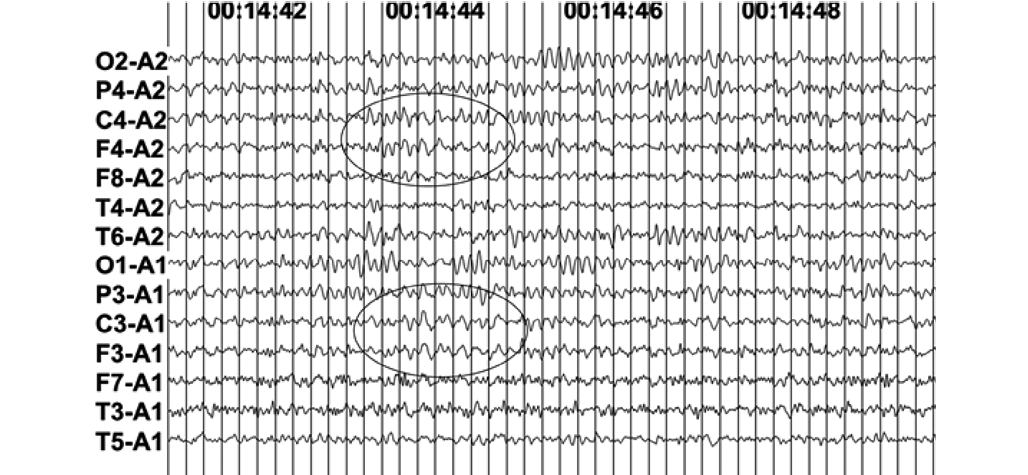
Some examples of bilaterally synchronous patterns of various origins are shown in Figures 1 and 2.
The table 5 shows the results of neuropsychological assessment resumed in profiles and their relation to individual’s EEG features.
It is important to underscore that the adolescents from the experimental group exhibited some similar and some different characteristics in both neuropsychological assessment and EEG analysis, that is, no single EEG pattern could be identified in adolescents from the ADHD group. With respect to the neuropsychological clinical profiles, it was also impossible to find a single correlation, however, certain regularities were observed. The majority of adolescents have shown difficulties with regulation, programming and control as unique characters or together with reduced level of general brain activation or difficulties of kinesthetic analysis and synthesis. Nearly all adolescents from experimental group have shown EEG patterns of suboptimal condition of hypothalamic structures, but always in combination with other deviated EEG patterns. Changes of hypothalamic genesis are rather frequently seen at adolescents’ EEG [Machinskaya, 2020] and associated with the activation of hypothalamo-pituitary system of hormonal regulation during puberty.
Table 5
Variants of neuropsychological and EEG profiles established
after qualitative analysis
of the data of adolescents with diagnosis of ADHD
|
Adolescents with diagnosis of ADHD |
Neuropsychological profile |
EEG profile |
|
Case 1 |
Deficit of regulation and control of activity |
1. Functional changes of hypothalamic genesis 2. Functional changes of basal ganglia genesis |
|
Case 2 |
Deficit of regulation and control of activity |
1. Functional changes of hypothalamic genesis 2. Functional changes of fronto-thalamic genesis |
|
Case 3 |
Deficit of regulation and control of activity |
1. Functional changes of hypothalamic genesis 2. Functional changes of basal ganglia genesis |
|
Case 4 |
Deficit of regulation and control of activity |
1. Slight functional changes of brainstem genesis 2. Slight functional changes of hypothalamic genesis |
|
Case 5 |
Deficit of regulation and control of activity |
1. Pronounced bilateral functional changes of fronto-thalamic genesis 2. Functional changes of hypothalamic genesis |
|
Case 6 |
Deficit of regulation and control and reduced arousal level |
1. Functional changes of hypothalamic genesis 2. Slight local changes (presumably of cortical genesis) in the left fronto-temporal area |
|
Case 7 |
Deficit of regulation and control and reduced arousal level |
1. Local slow wave changes in the left central and inferior frontal regions 2. Changes of limbic genesis 3. Functional changes of fronto-thalamic genesis 4. Functional changes of hypothalamic genesis |
|
Case 8 |
Deficit of regulation and control and reduced arousal level |
1. Functional changes of hypothalamic genesis 2. Functional changes of limbic genesis |
|
Case 9 |
Deficit of regulation and control and deficit of kinesthetic analysis and synthesis |
1. Functional changes of caudal brainstem genesis 2. Functional changes of hypothalamic genesis |
|
Case 10 |
Absence of neuropsychological profile |
1. Functional changes of mesencephalic genesis |
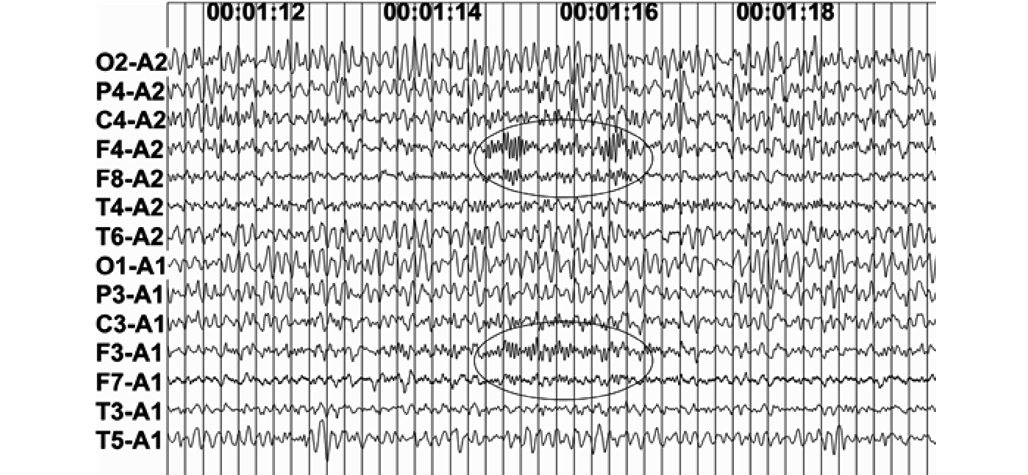
Fig. 1. An EEG segment shows bilaterally synchronous
beta — spindles (β) in frontal (F3, F4) and inferior frontal (F7, F8) leads.
The EEG pattern of suboptimal functioning of fronto-basal structures shown for
the case 3 with ADHD
(neuropsychological profile # 1: deficit of regulation and control)
(neuropsychological profile # 2: deficit of regulation, control and reduced arousal)
Analysis of results
Individual qualitative EEG analysis showed that the same behavioral (ADHD symptoms) and neuropsychological (deficit of voluntary regulation and control) manifestation could be associated with the suboptimal conditions of different cortico-subcortical regulatory systems. In analyzed cases, we found suboptimal functioning of fronto-thalamic system (cases 2, 5, 7), fronto-basal system (cases 1, 3), left fronto-temporal or left fronto-central regions (cases 6, 7). According to the clinical and neurophysiological data, all these functional systems participate in realization of voluntary control of goal-directed activity -executive functions- [Luria, 1966; Monchi, 2006; Nakajima, 2017].
Clinical neuropsychological profile 1 (deficit of regulation and control) was related to deviated EEG patterns of different origin: fronto-thalamic, limbic and basal-ganglia. All these patterns appeared together with hypothalamic patterns (5 cases). Clinical profile 2 (deficit of regulation and control and with lowing of the brain arousal level) was related to local EEG changes in anterior zones or EEG changes of caudal brainstem genesis (3 cases). Clinical profile 3 (deficit of regulation and control and kinesthetic integration) was related to abnormal EEG patterns of caudal brainstem genesis. In the case with clinical profile 4 (absence of neuropsychological syndrome), EEG traces showed functional changes of mesencephalic genesis.
In other words, it’s possible to say that the neuropsychological profile of difficulties of programming, regulation, and control might be recognized as a diagnosis of attention deficit disorder. Next in the order, the profiles of insufficient brain activation (low arousal level) might also be related to the diagnostic of attention deficit disorder. Both, the deficit of regulation and control and the deficit of general brain activation, are different neuropsychological profile in the qualitative approach [Luna-Villanueva, 2017; Ochoa, 2018]. At the same time, possible combinations of difficulties of programming and control together with difficulties of general brain activation or kinesthetic integration would be not taken into account without the application of qualitative analysis of errors during the neuropsychological assessment.
The study shows that adolescents diagnosed with ADHD exhibit heterogeneous clinical characteristics and certain similar regulatory traits. The external behavioral symptoms exhibited by these subjects are homogeneous in appearance alone since different brain functional mechanisms can be identified. These mechanisms can be assessed from at least two levels of analysis: clinical neuropsychological evaluation and EEG visual qualitative analysis.
According to our data, adolescents with ADHD can show different cognitive and behavioral problems. According to the conception or functional units of the brain [Ardila, 2020; Luria; Luria, 1966; Luria, 1973], these difficulties may be related to three systems or syndromic variants: 1) deficit of programing and control of voluntary activity (third functional block), 2) deficit of analysis and synthesis of somatosensory information (second functional block) and 3) low functioning of the brain activation systems (first functional block).
According to the qualitative approach, ADHD in preschool and school-age children is not a single clinical picture with unique neuropsychological and neurophysiological levels in all studied cases [Solovieva, 2013; Solovieva, 2016]. Neuropsychological difficulties such as functional impairment have been reported in different brain functional mechanisms such as mechanisms that regulate and control activity, integration of spatial information and insufficient activation of brainstem systems [Solovieva, 2016].
Different manifestations of ADHD are related to different conditions of subcortical brain levels that can manifest themselves heterogeneously at distinct periods of development. According to this assumption, multiple characteristics have been reported in brain regulation systems at different ages in preschoolers, primary students, and adolescents [Farber, 2015; Machinskaya, 2004; Machinskaya, 2014].
Moreover, EEG visual qualitative analysis made it possible to characterize the essential patterns of immaturity in the frontal-thalamic regulation system and deficit of non-specific regulation related to reticular formation at the brainstem level [Machinskaya, 2014]. These patterns are frequently observed in children diagnosed with ADHD at preschool age and older [Solovieva, 2013]. However, there are also cases in which other patterns of brain electrical activity have been observed [Solovieva, 2016].
Different electroencephalographic patterns were also detected in our study. With respect to the profile of deficit in regulation and control, variants in EEG functional changes were found at the basal ganglia, fronto-thalamic in different combinations and in constant combination with hypothalamic level. For the profile of deficit of regulation and control and the deficit of lowing of the brain arousal level, the changes were related to the limbic, frontal-thalamic, and hypothalamic system. In the case of this neuropsychological profile, we also found local changes in the left fronto-temporal area and in the left central and inferior frontal regions, according to EEG. As for the kinesthetic difficulties, regulation and control profile, the brainstem, and hypothalamus were found.
It is important to stress that combination of deviated EEG patterns of different origin with the pattern of hypothalamic genesis is typical for adolescence, as it wasn’t present so frequently in other ontogenetic periods [Machinskaya, 2020; Solovieva, 2016]. The physiological pattern of mesencephalic origin was observed in the adolescent with ADHD, where no neuropsychological patterns were detected. This underscores that the presence of electroencephalographic patterns does not necessarily determine a clinical picture. As such, EEG data cannot be used as a direct predictor of clinical difficulties, independently of neuropsychological assessment.
Recent studies show that the symptoms observed in ADHD did not show typical focal cortical changes, but rather diffuse and more global participation of subcortical regulation levels [Hoogman, 2017; Machinskaya, 2014; Solovieva, 2013; Solovieva, 2016]. These findings support Xomskaya’s [Xomskaya, 2002] hypothesis that the large areas of cerebral hemispheres with a complex organization of neural levels, cortico-cortical and cortico-subcortical relationships might participate as a morphological substrate of neuropsychological factors. However, one of the participants of our study has presented local changes of cortical genesis and another one local changes of subcortical genesis of frontal and fronto-central regions, both of them presented difficulties with programming, regulation and control and deficit of brain non-specific activation or arousal level. In both cases, additional patterns of brainstem level were also present.
Similar cases of suboptimal functioning of various parts of the brain regulatory systems (limbic, fronto-thalamic, fronto-basal, hypothalamic, etc.) according to the visual analysis of EEG traces, have been reported in adolescent with signs of behavioral and emotional problems at home and school [Machinskaya, 2014].
These findings support the idea that ADHD is not a single clinical picture since several neuropsychological profiles related to different brain systems were detected. Qualitative data suggest the necessity of an individual approach for the precision of brain mechanisms or neuropsychological factors in each concrete case [Solovieva, 2020].
The mentioned data question the importance of focusing on external behavior as the only level of analysis in clinical psychiatry, where the diagnosis is established based on the caregiver’s answers in the interview [Wang, 2017]. This type of diagnosis, which is used predominantly by specialists in most countries, should be subjected to reflective criticism.
Thus, it can be concluded that the behavioral approach of DSM-5 [American Psychological Association] does not completely explain the possible causal mechanisms of ADHD. This agrees with some authors, who indicate that diagnosis based on interview data does not identify the etiology of the disorder or propose a justifiable intervention [Thome, 2012; Wang, 2017]. Our new data allow noticing that diagnosis of attention deficit disorder might include adolescents with the deficit of regulation and control and the deficit of general brain activation, the combination of these both deficits and also other possibilities of deficits, for example, the deficit of kinesthetic integration. Even adolescents with the absence of any kind of neuropsychological profile might receive a diagnosis with attention deficit disorder [Solovieva, 2017a].
It is important to underscore that the supposition about the unique behavior of ADHD has been disseminated by DSM-5 [American Psychological Association] and widely reproduced by health professionals, schools and families. Some authors such as [Koutsoklenis, 2019] report that understanding ADHD is influenced by the social, and cultural ideas about “normal development” and the “idealized child”, in which the emphasis on management of this entity is the responsibility of schools and education.
At the same time, there is a new tendency to move the DSM’s diagnostic criteria towards a dimensional approach. The World Psychiatric Association created a Research Domain Criteria (RDoC) initiative for research purposes, with the aim to develop new ways of classifying mental disorders based on a matrix of dimensions -neurobiological, and cognitive mechanisms, social processes, arousal and regulatory systems-, because advances in integrative neuroscience were not being applied in patient care [Sanislow, 2016].
In our study, the qualitative analysis shows a set of clinical variables that have predictive value for detecting a neuropsychological profile in ADHD, such as deficit in regulation and control and low level of general brain activation. At the same time, some specific variants (deficit in kinesthetic integration or combinations of deficits) might be lost in case of the absence of qualitative neuropsychological analysis. Additionally, the analysis of EEG shows the predominant role of subcortical origin (functioning pattern most prominent) of the difficulties traditionally associated with the diagnosis of ADHD. That finding indicates the value of applying qualitative diagnostic methods in two levels, such as neuropsychological assessment and EEG in the analysis of brain functional mechanism of difficulties in adolescents.
It can therefore be hypothesized that what is occurring with the diagnosis of ADHD is that children and adolescents with different qualitative characteristics are being included in the same clinical group for no clear reason. Such a fact might be related to exclusive consideration of quantitative criteria and the interview method as a unique method for assessment.
It could be said that the traditional approach in psychology, medicine and neuropsychology has taken ADHD as a “thing” and has not examined the process or the precise functional characteristics in the subjects [Vigotski]. Studies, from cognitive quantitative approach, have been interested in establishing external descriptive signs of external behavior, rather than precise neuropsychological mechanisms and their dynamic manifestations at different ontogenetic stages. Furthermore, the study of the influence of the academic-educational environment on adolescents with ADHD, as well as the reflexive analysis of diagnostic systems, cannot be conceived outside the scope of the clinical perspective of cultural historical neuropsychology [Luria, 1966; Solovieva, 2020; Vigotski].
The limitations of the study might be related to the necessity of special professional preparation of researchers. In order to reproduce the procedures of this investigation, professionals and researchers must be trained in the theoretical and clinical principles of qualitative neuropsychology. Future research dedicated to adolescents with ADHD within qualitative neuropsychology should be focused on the relation between clinical profiles reported in this study and academic performance in math, reading, and writing tasks. It’s also necessary, to provide studies in this population on the design and approval of programs of neuropsychological intervention with the validation of their effectiveness.
Conclusions
In studied adolescents, the diagnosis of ADHD did not indicate the existence of a homogeneous group in terms of neuropsychological and neurophysiological analyses. The behavioral reports obtained in the caregivers’ answers to the initial interview questions are only the starting point for the syndromic study of ADHD. The contribution of this study lies in the establishment of accurate neuropsychological criteria for ADHD, using the qualitative approach, as the basis for guiding measures and designing specific intervention programs for these cases.
The search for usage of different levels of analysis such as electrophysiological and neuropsychological assessment might therefore become an interdisciplinary heuristic model for the accuracy of underlying brain functional mechanisms in students with similar and different symptoms due to distinct causes.
Thus, the psychological development in these cases, in particular of the regulation and control systems, must be formed in adolescents with the participation of the adult, teacher or health professional, based on the design of appropriate pedagogical and treatment strategies. At the family level it might also be decisive to foment parenting models aimed at activity of planning and organization of communicative and intellectual activities. The progressive formation of psychological processes in accordance with the gradual internalization of external social interactions is one of the essential postulates of the cultural-historical approach in psychology and is also essential for the field of clinical neuropsychology.
The paper recognizes the value of the qualitative procedure developed by L.S. Vygotsky and A.R. Luria as an alternative approach for the analysis of the difficulties shown by adolescents with ADHD in determining their psychophysiological mechanisms. Such an approach can help to establish guidelines and strategies for neuropsychological, psychological and pedagogical treatment in each particular case. The authors assume the cultural-historical approach for the design of the research, the development of a qualitative evaluation at different levels of analysis: neuropsychological and electroencephalographic, as well as to position some criticisms to the current problematic of ADHD studies.