INTRODUCTION
Azerbaijan is an upper-middle-income country in the South Caucasus region with a population of approximately 10 million and a prevalence of urban residency. The gross domestic product (GDP) per capita in 2020 was US $ 4,214.31, and where 3.5% of GDP was allocated to healthcare [1]. Although mental disorders contribute to 9.1% of Disability Adjusted Life Years (DALYs), mental health expenditure accounts for only 3.4% of the general health budget [2].
The healthcare system is currently in the process of large-scale reform as a result of which the majority of medical services were transferred to State Agency on Mandatory Health Insurance (SAMHI) financing, though certain facilities still continue to be financed by the Ministry of Health (MoH). The consequences of this separation have been most pronounced for mental health services: psychiatric hospitals and specialized outpatient centers are managed by the MoH, and mental health services in general health settings are assigned to the SAMHI. In this regard, mental health care provision has a significant number of conflicting approaches that influence decision-making processes. For example, improved access to community-based services is acknowledged to represent a better alternative to institutionalization; however, only 15% of the mental health budget is allocated to outpatient care. Another example is a general recognition of the need to introduce a multidisciplinary approach in care provision, but rate at which new positions are becoming available for mental health professionals is extremely slow. Development of community-based mental health services requires effective collaboration not only within the healthcare sector, but also with other stakeholders, in particular social welfare and education [3]. Unfortunately, mental disorders and mental disability are still managed from within the framework of a rigid medical-centered model that effectively prevents the delivery of comprehensive care, including psychosocial interventions, sheltered housing, vocational training, supported employment, etc. In the absence of well-developed social services, most people with mental illness have reported unmet needs with regard to their daytime activities, occupations, and socialization [4].
Despite these difficulties, the mental health system’s transition from an institutional model to community-based care continues. In recent years, the government implemented important initiatives in mental health to meet modern requirements in care provision.
The aim of this article is to review the transformation of mental health care, describe organizational model in mental health, indicate the advantages and disadvantages of existing services, and discuss the principal lessons learned in the course of such mental health reform.
BRIEF HISTORICAL PERSPECTIVE
The first psychiatric hospital, which consisted of just 30 beds, was opened as a charity initiative in Baku in 1892. In the first half of the 20th century, various attempts were made to open new psychiatric facilities in the framework of the formation of the Soviet healthcare system. However, the establishment of psychiatric hospitals was slow because of a lack of professionals in the field, and hence there were two psychiatric facilities in the capital and a few psychiatric wards scattered around general hospitals in the regions [5].
The introduction of psychopharmacotherapy in the early 1960’s resulted in the development of eight new mental health settings (so-called inter-regional psycho-neurological dispensaries) providing both in-patient and out-patient treatment. In the 1970s and 1980s, there was a record increase in the number of beds, achieving a maximum of 2265 beds in the largest psychiatric hospital. At the same time, excessive institutionalization in mental health went hand-in-hand with certain destructive effects such as segregation of psychiatric services from general healthcare, patients’ isolation from society, deteriorating quality of services, and systematic human rights violations [6].
The restoration of independence in 1991, accompanied by the Karabakh War, resulted in an enormous inflow of refugees, and a severe economic crisis resulted in the collapse of the mental health system in Azerbaijan [7]. Over subsequent decade, these services remained disproportionately institutionalized, over-centralized, underfinanced, and restricted in terms of the available range of services [8].
The adoption of the first piece of legislation on psychiatric care in 2001, and the assessment of the mental health system conducted by the World Health Organization (WHO) in 2007, triggered a broader discussion on the reformation of mental health services in the country [9]. The subsequent decisions mainly affected in-patient facilities through improvements to living conditions, and the supply of medicines and food. In addition, the number of psychiatric beds was reduced from 73.9 to 38.3 per 100,000 [10].
With the view of taking forward the mental health reform, the MoH established a taskforce including mental health professionals, representatives of health administration, and social activists. The taskforce developed the National Mental Health Strategy and Action Plan, which came into effect in 2011 [11]. These documents focused on human rights protection, enhancing governance and intersectoral coordination, building capacities in mental health, improving quality of services, and implementing new services, as well as integrating mental health into general healthcare. In line with these documents, the National Assembly amended the Law on Psychiatric Care to entitle primary care doctors to treat common mental disorders. The MoH developed the relevant clinical guidelines and provided appropriate training for general practitioners.
In addition, with the aim of strengthening psychosocial support in Azerbaijan, the Law on Social Services and the Law on Psychological Care were adopted in 2017 and 2019, respectively. Along with the development of national legislation over the years, Azerbaijan has joined international agreements such as the UN Convention on the Rights of Persons with Disabilities, the WHO Mental Health Declaration for Europe, and the Comprehensive Mental Health Action Plan 2013–2030.
ORGANIZATION OF MENTAL HEALTH CARE SYSTEM
National Mental Health Centre
The National Mental Health Centre (NMHC) was established in 2012 within the framework of the mental health reform. The NMHC structure consists of the Organization and Programs Department, Emergency/Crisis Intervention Unit, Outpatient Unit, Psychosocial Rehabilitation Unit, Child/Adolescent Mental Health Unit, and Daycare Unit.
The NMHC is responsible for the stewardship and coordination of mental health services at the national level. These responsibilities include governance, monitoring and quality assurance for mental health care, as well as analysis of mental health statistics, drafting policy documents (e.g., special programs, practice guidelines, and reports), and providing expert advice for the government. Since a significant number of mental health services are offered by the SAMHI and the Ministry of Labor and Social Protection, the NMHS actively cooperates with these bodies to address mental health issues (Figure 1).
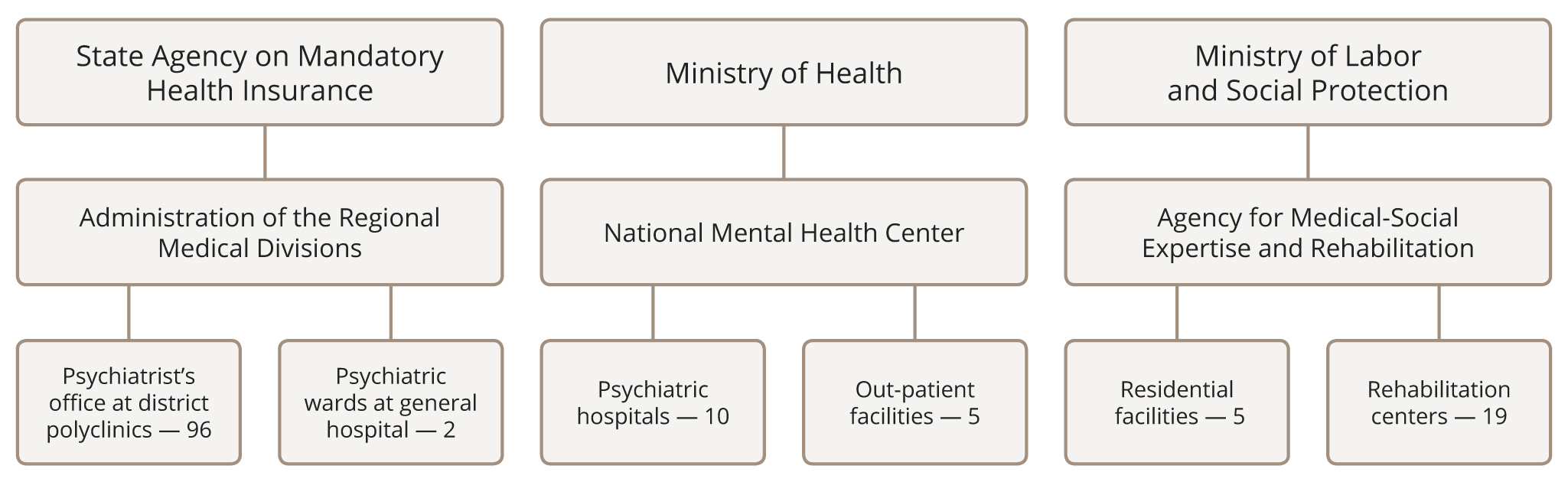
Figure 1. Organizational structure of mental health care in Azerbaijan.
Furthermore, the NMHC develops new approaches to care provision through planning and implementation of community-based services in different regions of the country. Another important activity is the strengthening of human resources via educational programs, training mental health professionals, and collaboration with academic institutions and international organizations.
Psychiatric hospitals
Inpatient treatment is provided by ten psychiatric hospitals subordinated to the MoH. Two hospitals are located in the capital, while the others are unequally distributed across the country. The number of psychiatric beds is sufficiently modest at 38.3 per 100,000 (Table 1), as compared to other post-Soviet countries at 79.6 per 100,000 [12].
Table 1. Mental health resources in Azerbaijan (per 100,000 of population)
|
Mental health staff |
Rate per 100,000 population |
|
Psychiatrists |
4.1 |
|
Psychiatric nurses |
7.8 |
|
Psychologists |
1.2 |
|
Social workers |
0.3 |
|
Inpatient facilities |
|
|
Number of psychiatric beds |
38.3 |
|
Number of admissions |
115 |
|
Out-patient facilities |
|
|
Number of visits |
1964 |
Most psychiatric hospitals have been renovated or rebuilt as a part of the mental health reform. The average length of stay in the hospital is approximately 60 days, and involuntary treatment makes up 9% of admissions [13]. In 2017, as survey undertaken within the WHO project on adults with mental disabilities living in institutions in the European Region revealed certain deficiencies in psychiatric hospitals [14]. These deficiencies included an absence of any well-defined procedures for discharging patients who have lost family and social ties, a lack of access to free legal representation by a lawyer and/or a social worker, a paternalistic approach (e.g., most decisions are psychiatrist-led rather than patient-led or shared), and insufficient coordination between services beyond healthcare.
Outpatient mental health centers
People with severe mental disorders who do not need acute inpatient treatment receive care at the five outpatient mental health centers available in Azerbaijan’s largest cities, where the range of services provided varies significantly from one center to another. Some centers focus on drug treatment and expert examination only, while others offer multiple services including daycare treatment, psychotherapy, and rehabilitation. All outpatient mental health centers are subordinated to the MoH and therefore have a well-established referral system with psychiatric hospitals. Until recently, the centers supervised the work of psychiatrists at district outpatient settings, but subsequent to the division of authority between the MoH and SAMHI, their supervisory functions have gradually diminished.
Psychiatrist’s office at district outpatient settings
In 2011, with the aim of integrating mental health services into the primary care system, psychiatric dispensaries were closed, and psychiatrists and psychiatric nurses transferred to primary care facilities. Thus, with mental health services being brought closer to the populace, access for patients with both mental and physical disorders has significantly improved, and the stigma associated with psychiatric treatment has in some way decreased. An psychiatrist’s office is now available in almost all outpatient healthcare settings (polyclinics) in each administrative district of the country. Since district outpatient settings have been organized on the basis of catchment areas, a psychiatrist’s office will typically provide services for 50,000 to 150,000 inhabitants. Just like all other primary health services, psychiatrists’ offices fall under the authority of the SAMHI.
Residential facilities
The capacity at residential facilities in Azerbaijan is 18.4 per 100,000, which is the lowest amongst all other countries of the WHO European Region [15]. There are only five residential facilities managed by the Ministry of Labor and Social Protection and, according to the existing regulations, they are intended for individuals officially recognized as persons with disabilities. Furthermore, people with mental disabilities are rarely admitted to such facilities due to staff concerns about problematic behaviors and limited opportunities for medical treatment. Therefore, up to 11% of patients lacking family and social ties have to stay in psychiatric hospitals after termination of acute in-patient treatment [16]. Presently the government has initiated discussions to arrange for sheltered accommodation for homeless people with mental illness, allowing for their earlier discharge from hospitals.
Rehabilitation services
Along with rehabilitation programs implemented by the MoH, there are 19 rehabilitation centers within the Ministry of Labor and Social Protection. Fourteen centers intended for adults and five centers for children are located in different regions of the country. Only patients with officially recognized disabilities can be admitted to the centers, and their referrals are coordinated with healthcare settings. Although the centers do not specialize according to form of disability, they employ mental health professionals to provide psychosocial interventions.
DEVELOPMENT OF COMMUNITY MENTAL HEALTH SERVICES
Until 2011, community mental health services were virtually non-existent in Azerbaijan. It may be noted that stand-alone initiatives were run by a number of non-governmental organizations, but which ultimately saw no sustainable success due to termination of their activities as soon as the donor’s funding ended. The idea of transition from institutional to community-based care was first mentioned in the National Mental Health Strategy. Chapter III Strengthening measures on prevention of mental health problems among population of the Strategy included a paragraph on establishing community mental health services [11]. The follow-up activities marked the beginning of the provision of community care.
Due to the lack of mental health professionals other than psychiatrists and psychiatric nurses, the government created jobs for clinical psychologists, social workers, and occupational therapists at healthcare facilities. In addition, newly recruited specialists were offered the opportunity to undergo professional training, either in the country itself or, indeed, abroad.
Between 2012–2014, the European Union sponsored the Empowerment of Mental Health Service Users in Five Regions of Azerbaijan project run by the Lithuanian non-governmental organization, Mental Health Perspectives. The project focused on developing community-based mental health services, psychosocial rehabilitation, human rights, and mental health users’ movements. Within the framework of the project, a large group of mental health professionals went to Lithuania to acquaint themselves with community mental health settings. In turn, international experts visited Azerbaijan to promote the development of modern, comprehensive services.
The most important tasks in launching community-based care have been assigned to the NMHC. In recent years, the NMHC dedicated significant effort to the deinstitutionalization of mental health care. It should be noted that the wide range of mental health programs, which included programs on psychosocial rehabilitation, case management, family support, and early intervention, were elaborated upon by the NMHC specialists. Subsequently, these programs have been translated into practice for inpatient and outpatient facilities.
In 2017–18, the MoH established 14 community-based mental health services for children and adolescents. These services were placed at district child outpatient healthcare facilities (child polyclinics) in various regions of Azerbaijan. The newly established services utilize a multidisciplinary approach provided by teams consisting of child specialists with a variety of professional backgrounds. Such a team would include a child psychiatrist, developmental psychologist, educational specialist, speech therapist, occupational therapist, and volunteers, who may be also parents of children receiving care.
In 2021, after the second Karabakh War, the government established community-based mental health services for veterans, family members of deceased servicemen, and war-affected civilians. These services were created within general health outpatient settings and mainly employed psychiatrists and psychologists to provide psychotherapy, crisis intervention, and drug treatment for people with post-traumatic stress disorder (PTSD) and other war-induced mental disorders.
Between 2020–2021, COVID-19 seriously affected community-based services in terms of reallocation of funding and restricted access to mental health care. Many outpatient settings were postponed or had their services reduced due to strict quarantine measures. All group activities conducted by mental health teams were canceled. At the same time, mental health services shifted to new modes of care delivery via telephone or online formats. As soon as restrictions associated with the pandemic were eased, these community-based services restored the full range of their activities.
STRENGTHS AND WEAKNESSES OF COMMUNITY-BASED CARE
Despite there being a relatively short history of community mental health services in Azerbaijan, one can see their undeniable advantages over institutional care. Community-based care seems to be efficient in terms of addressing the populace’s needs in ways that are both accessible and acceptable [17]. Patients with severe mental disorders who were being treated in traditional psychiatric facilities had increased the number of unmet needs as compared to patients with the same diagnoses receiving community mental health services [18]. As predicted, patients reported greater satisfaction with mental health services in the community settings, which they found to be comprehensive, person-centered, and recovery-oriented [19]. In recent years, significant progress has been observed in the implementation of psychological interventions and psychosocial rehabilitation. Many people with mild to moderate mental disorders have been able to benefit from counselling sessions, and individual and group psychotherapy, while patients with severe mental disorders have been able to gain access to and participate in rehabilitation programs [20]. There is also evidence to suggest that drug prescription in community mental health settings better meets clinical guidelines than the treatment provided by traditional psychiatric institutions [21].
Although community-based care is considered to be less stigmatizing, that stigma that remains associated with mental disorders still prevents patients from applying for services and contributes to the low priority the government currently assigns to mental health. The above-mentioned distribution of authority in mental health care between the MoH and the SAMHI do not promote community care’s ability to address the needs of people with severe mental disorders because of significant differences in the understanding of goals, approaches, and decisions in the field of mental health by each of these authorities. On the one hand, the SAMHI administration is responsible for primary healthcare and interested in preventing most common mental disorders, while treatment of severe mental disorders remains underestimated and unaddressed; on the other, the MoH is mainly responsible for the treatment of individuals with mental disabilities, but have significantly lower financing and other resources with which to establish community-based services. These contradictions may be resolved through certain boundaries determining roles and competencies between the two health authorities, as well as improving their coordination and cooperation.
Due to a shortage of psychiatrists and other mental health professionals, especially in the regions, most mental health services are concentrated in large cities and are barely accessible, or indeed affordable, for people living in rural areas.
Notwithstanding these challenges, development of mental health care is becoming increasingly important, as evidenced by its inclusion in the Principles of the Sustainable Development Goals (SDGs) [22]. Azerbaijan, as a member country, has prioritized SDGs and their targets indicators, including those addressing mental health. In 2021, the government, in cooperation with non-governmental and international organizations, established the Mental Health and Psychosocial Support Technical Working Group. This provided a platform for better coordination and focused inter-agency responses to mental health needs, the implementation of standards of best practice and global interagency recommendations, and the promotion of the quality of psychosocial interventions through joint capacity-building activities.
CONCLUSIONS
The model of mental health services in Azerbaijan represents a quaint combination of institutionalized inpatient care, and outpatient psychiatric counselling and treatment that is semi-integrated into primary healthcare and the recently established community-based mental health services. Due to an absence of a unified systematic approach to mental health services, the community care provided by the healthcare and social welfare systems remains fragmented, poorly coordinated, understaffed, and underfinanced. Nevertheless, we can see a significant shift in paradigm as a result of the increasing attention being paid to mental health issues by policymakers, the media, and the general public. Community-based mental health services have been the subject of discussion at all levels of health and social welfare authority. Moreover, representatives of international organizations in Azerbaijan, such as the WHO, UNICEF, and the International Committee of the Red Cross (ICRC), actively promote programs to develop community-based services for vulnerable adults and children.
At present, one important task facing the healthcare system is the switch from conventional indicators (e.g., the number of inpatient admissions and discharges, number of outpatient visits, etc.) to service outcome indicators (e.g., functioning level, quality of life, and satisfaction with care). In this regard, planning and implementation of mental health policy based on service outcomes opens up vast prospects for the development of community services in Azerbaijan.