Introduction
Global population ageing is one of the key demographic challenges facing contemporary society. According to the World Health Organization, by 2030 one in six people worldwide will be over the age of 60, and by 2050 the number of individuals in this age group will reach 2.1 billion1. Increased life expectancy is accompanied by a growing prevalence of age-related cognitive impairment, including dementia, which places a substantial burden on healthcare and social support systems2.
In this context, the concept of healthy (normative) ageing becomes particularly important, as it emphasizes the maintenance of functional capacity and quality of life in later life3. However, normative ageing is not a completely deficit-free process. Even in the absence of clinically significant cognitive impairment, age-related changes are observed in information processing speed, working memory capacity, and cognitive flexibility (Harada, Natelson Love, Triebel, 2013; Salthouse, 2010; Prince et al., 2024). Age-related changes in cognition and behaviour are highly heterogeneous in their timing and follow an individual developmental trajectory. The most prominent changes are associated with the neuropsychological factor that is most sensitive to increased cognitive load (Roshchina, 2015). These changes occur alongside the activation of compensatory mechanisms; they reflect a decline in the efficiency of neural networks and may increase vulnerability to cognitive decline in the long term.
At the same time, contemporary neurocognitive models of ageing emphasise the preservation of a certain degree of neuroplasticity in later life, making it possible to influence cognitive processes through targeted, structured interventions (Prince et al., 2024). In addition to somatic diseases, visual and hearing impairments, and unhealthy habits, risk factors for cognitive decline in ageing include a low level of education as well as insufficient cognitive, physical, and social activity (Roshchina et al., 2022; Tkacheva et al., 2021; Colita et al., 2024; Livingston et al., 2024; Tong et al., 2025). The likelihood of developing clinically significant cognitive impairment increases when the neuropsychological factor most sensitive to cognitive decline is exposed to a greater functional load in the context of insufficient cognitive reserve (Tretyakova, Pultsina, 2024; Cherdak, 2023; Roshchina, 2015).
Against this background, increasing attention is being paid to the development and evaluation of preventive interventions aimed at maintaining cognitive functioning in older adults without significant cognitive impairment. Current recommendations emphasize the importance of cognitive, physical, and social activity as factors contributing to the preservation of cognitive health4 (Livingston et al., 2020). At the same time, despite the growing number of studies, evidence regarding the effectiveness of structured cognitive interventions in populations experiencing normative ageing remains inconsistent.
Clinical guidelines in many countries, including those issued by the Ministry of Health of the Russian Federation, identify cognitive stimulation and cognitive training as key non-pharmacological strategies for preventing cognitive decline and supporting both older adults experiencing normative ageing and individuals at increased risk5.
Given that age is the primary risk factor for cognitive decline, while modifiable behavioural and social factors substantially influence trajectories of cognitive ageing (Roshchina et al., 2022; Cherdak et al., 2024; Colita et al., 2024; Tong et al., 2025), the use of structured cognitive stimulation programmes in populations experiencing normative ageing appears to be a promising approach for maintaining cognitive reserve and reducing the risk of further cognitive decline.
At the same time, meta-analytic reviews indicate that cognitive training may lead to improvements in specific cognitive functions, primarily within the domains being trained (Lampit, Hallock, Valenzuela, 2014; Velloso et al., 2025). However, the extent to which these effects transfer to everyday functioning and quality of life, as well as their long-term sustainability, remains a matter of debate. Furthermore, relatively less attention has been paid to interventions that integrate cognitive, social, and emotional components, despite their potential importance in the context of healthy ageing.
Cognitive Stimulation Therapy (CST) is a structured group intervention originally developed for individuals with mild to moderate dementia and aimed at maintaining and improving cognitive functioning and quality of life (Orrell et al., 2017; Spector et al., 2003).
Meta-analyses and review studies have shown that the standard 14-session CST protocol leads to significant improvements in cognitive performance, affective regulation, and quality of life (Aguirre et al., 2013; Orrell et al., 2017). CST has been incorporated into international clinical guidelines (including those issued by the National Institute for Health and Care Excellence NICE, UK) as one of the core non-pharmacological interventions for mild to moderate dementia. Evidence is also available regarding the application of CST protocols in individuals with mild cognitive impairment (Desai et al., 2024). Participants who completed cognitive stimulation programmes demonstrated improved cognitive status and reduced apathy compared to control groups (Chen et al., 2025; Desai et al., 2024).
Furthermore, CST has been successfully implemented across a wide range of organisational settings, including nursing homes, day-care centres (Fisher et al., 2025), and outpatient memory clinics, as well as in adapted formats delivered by nursing staff and other non-specialist practitioners. This demonstrates the high scalability and flexibility of the intervention (Aguirre et al., 2013; Desai et al., 2024).
A substantial body of research on non-pharmacological interventions in cognitively healthy older adults indicates that cognitive stimulation, as a class of interventions, is both feasible and appropriate for use in normative ageing. Systematic reviews have reported small but consistent effects on memory, attention, executive functions, and overall functioning (Apóstolo et al., 2019; Mowszowski et al., 2016; Tardif, Simard, 2011; Velloso et al., 2025b). A review of programmes designed for healthy older adults emphasises that cognitive stimulation, as a form of structured multidimensional activation of cognitive processes, constitutes an appropriate and safe intervention for normative ageing, rather than only for individuals with existing cognitive impairment (Tardif, Simard, 2011). Moreover, recent studies, including focus group research, have demonstrated a substantial demand among cognitively healthy older adults for programmes similar in structure to CST but oriented towards the goals of active ageing, including maintaining autonomy, preventing cognitive decline, and enhancing social participation (Velloso et al., 2025a; Velloso et al., 2025b; Coşkun, İnel Manav, 2025).These findings suggest that CST may be viewed not only as a therapeutic intervention for cognitive decline, but also as a model of structured cognitive activity that may be effective in maintaining cognitive reserve and preventing cognitive deterioration in the context of normative ageing (Tardif, Simard, 2011).
The present study builds upon and extends a line of research focused on the implementation and adaptation of Cognitive Stimulation Therapy (CST) within Russian practice. In 2024, a comprehensive cultural adaptation of the CST protocol for a Russian-speaking sample of older adults with cognitive impairment was conducted, the results of which are presented in detail elsewhere (Shvedovskaya et al., 2024). The adaptation process followed the international FMAP (Formative Method for Adapting Psychotherapy) framework, which enabled not only the translation and cultural adaptation of the group facilitator’s manual, but also its expert evaluation and pilot implementation in a residential care facility. The findings demonstrated high acceptability of the programme, its feasibility in the Russian context, and positive subjective evaluations from both participants and group facilitators. Importantly, the previous study focused on the clinical effectiveness and feasibility of CST among individuals with cognitive impairment. The scientific novelty of the present study lies in the first empirical evaluation of the applicability and feasibility of the adapted Russian CST protocol in the context of normative ageing.
Accordingly, the aim of the present study was to evaluate the applicability and feasibility of the Cognitive Stimulation Therapy (CST) programme in the context of normative ageing.
The pilot study addressed the following research questions:
RQ1: How do older adults with normative ageing who participate in the CST programme evaluate its effectiveness and their level of satisfaction with the sessions?
RQ2: What effects does the CST programme have on cognitive functioning and quality of life in older adults with normative ageing?
RQ3: What modifications to the CST programme could be proposed to optimise its implementation for older adults with normative ageing?
Materials and Methods
A pilot pre–post study was conducted to evaluate the feasibility of the Cognitive Stimulation Therapy (CST) programme and to obtain preliminary data on its potential effects on cognitive functioning and quality of life indicators in individuals experiencing normative ageing.
Sample Characteristics
The study included 10 participants aged 59 to 81 years (mean age = 70.2 ± 6 years), including one man and nine women. Nine participants had completed higher education, while one had completed secondary vocational education. The inclusion criteria were: absence of diagnosed neurological or psychiatric disorders; absence of chronic conditions affecting cognitive functioning; and absence of clinically significant cognitive impairment, as confirmed by normative scores on the ACE-III (≥ 82 points).
Participation in the CST programme was voluntary. All programme participants were enrolled in the Moscow Longevity project. This project is open to Moscow residents who have reached pre-retirement age (women aged 55 years and older and men aged 60 years and older). Participants registered for the in-person Cognitive Stimulation Therapy course offered as part of the ongoing educational workshop Brain Gym. Sessions were conducted at Moscow State University of Psychology and Education between October and December 2025.
Of the 10 subjects who initially responded to the invitation to participate in the programme, five withdrew after the initial assessment and receiving detailed information about the format of the sessions. Data obtained from the initial survey of these five subjects were used to analyze potential factors associated with participation in or withdrawal from the programme.
Reasons for non-participation were collected through a questionnaire and grouped into several categories:
- Mismatch between the programme and participants’ expectations: “I thought cognitive abilities meant solving tasks and doing exercises (for example, finger exercises). I was prepared for that. But talking and discussing things was not really what I was looking for. Not because it was bad — I simply expected one thing and encountered something different”.
- Lack of interest in this type of activity: “I am about to turn 69, and I am not at that stage yet… I understand the idea behind your approach — throwing a ball and retrieving words from memory (beetroot, borscht). But at the stage I am currently at, everything is fine with me”.
- Practical barriers to participation (location and transportation difficulties): “The venue is very far from where we live; we live in remote districts compared to the meeting location. We overestimated our capabilities”; “An hour and a half each way during rush hour is simply too much”.
- Preference for other types of activities: “Your group is very useful for people who live alone, but I live with my husband, so it is not really for me”; “I expected memory-training techniques and thought the programme would be more challenging”.
Thus, the final intervention group consisted of five participants aged 59 to 81 years (mean age = 71 ± 8.1 years), including one man and four women.
Intervention
The programme content followed the standard CST protocol (Shvedovskaya et al., 2024). The intervention consisted of 14 thematically structured sessions. Sessions were conducted twice weekly, and the sequence of topics specified by the programme developers was strictly followed. Each session lasted between 60 and 90 minutes. Each session comprised three components: an introductory part (greeting, warm-up activities, and discussion of current events), a refreshment break, and a main part consisting of one to three activities related to the session theme. The session concluded with a closing component that included singing a song, completing a feedback questionnaire, and introducing the topic of the next session. The group was led by two permanent facilitators, with the assistance of one or two additional staff members. Certain elements of the programme were adapted to reflect the characteristics of a normative ageing sample, including increased cognitive demands and a reduction in excessive detail in some programme components (Appendix, Table).
Measures
Assessment was conducted at two time points: before the start of the programme and after its completion.
Cognitive functioning was assessed using the Addenbrooke’s Cognitive Examination III (ACE-III), which provides an evaluation of overall cognitive functioning and enables the construction of a neuropsychological profile across the domains of attention, memory, verbal fluency, language, and visuospatial abilities (Varako et al., 2022; Varako et al., 2024).
Subjective quality of life was assessed using the SF-36 Health Survey, which includes scales measuring physical and mental health components, including physical functioning, role functioning, social functioning, vitality, and mental health (Novik, Ionova, 2021; Smirnova, Krutko, Belova, 2021; Ware, Sherbourne, 1992).
Throughout the programme, participant feedback was collected after each session using a questionnaire. The questionnaire comprised three sections: a quantitative evaluation of the session (interest and satisfaction), an open-ended question regarding the most enjoyable aspects of the session, and an open-ended question concerning possible improvements. Questionnaires were completed individually in paper-and-pencil format immediately following each session.
Participant progress and engagement were also monitored during each session using the following parameters: interest, communication, enjoyment, and mood. Observation forms for each participant were completed after every session based on a joint discussion among the facilitators.
Subjects who completed the initial assessment but declined participation in the programme were interviewed regarding their reasons for non-participation using a semi-structured interview.
Data Analysis
Given the small sample size, the analysis primarily focused on descriptive statistics, the examination of individual trajectories of change, and the estimation of effect sizes in order to evaluate the feasibility of CST in a normative ageing sample. Changes between the two assessment time points were analyzed using Student’s paired-samples t-test and the Wilcoxon signed-rank test. Effect sizes were estimated using Cohen’s d for the t-test and the rank-biserial correlation coefficient (rbc) for the Wilcoxon test. Statistical significance was considered as a secondary indicator, as the pilot nature of the study and its limited sample size did not provide sufficient statistical power to support definitive conclusions.
Feasibility of the programme was evaluated using a combination of behavioural and subjective indicators reflecting both the implementation process and participants’ perceptions of the intervention. The key indicators included recruitment, reflecting the accessibility and attractiveness of the programme; retention, indicating the sustainability of participation; attendance, reflecting actual engagement in programme activities; acceptability, referring to participants’ evaluations of the programme; and adherence, reflecting the extent of active participation throughout the intervention.
Operational indicators included the proportion of participants who completed the programme, the number of sessions attended, satisfaction ratings, and qualitative participant feedback obtained through the session evaluation questionnaires.
Results
Of the ten subjects invited to participate in the programme, five (50%) enrolled in the intervention. Participant retention was high, reaching 100%, as all five subjects who began the programme completed it. The number of sessions attended ranged from 9 to 14, with a median attendance of 11 sessions. Participant satisfaction with the programme was also high. Mean satisfaction scores across the 14 sessions ranged from 3.83 to 4.00, with an overall mean score of 3.93 out of 4. More than 90% of all ratings were the maximum possible score.
To assess changes in cognitive functioning among programme participants, mean scores on the Addenbrooke’s Cognitive Examination III (ACE-III) and the SF-36 Health Survey obtained before and after the intervention were compared. The results are presented in Table 1.
Table 1
Comparison of mean ACE-III and SF-36 scores at two time points
|
Scale |
Mean (SD) |
t-test result |
Wilcoxon test result |
|
|
Time point 1 |
Time point 2 |
|||
|
Addenbrooke’s Cognitive Examination (ACE-III) |
||||
|
Attention |
17.6 (0.548) |
16.8 (1.643) |
t(4) = 1.206, p = 0.294, d = 0.539 |
W = 8, p = 0.345, rbc = 0.6 |
|
Memory |
24.6 (0.894) |
24.6 (1.14) |
t(4) = 0, p = 1, d = 0 |
W = 5, p = 1, rbc = 0 |
|
Associative processing speed |
9.6 (2.966) |
10.8 (2.28) |
t(4) = -2.449, p = 0.07, d = -1.095 |
W = 0, p = 0.089, rbc = -1 |
|
Language |
24 (1.581) |
24.8 (1.643) |
t(4) = -1.089, p = 0.338, d = -0.487 |
W = 1, p = 0.423, rbc = -0.667 |
|
Visuospatial functions |
14.6 (1.14) |
14.6 (1.14) |
t(4) = 0, p = 1, d = 0 |
W = 3, p = 1, rbc = 0 |
|
Total score |
90.4 (3.715) |
91.6 (4.159) |
t(4) = -1.5, p = 0.208, d = -0.671 |
W = 1.5, p = 0.265, rbc= -0.7 |
|
Quality of Life Questionnaire (SF-36) |
||||
|
Physical functioning |
86 (10.84) |
86 (8.22) |
t(4) = 0, p = 1, d = 0 |
W = 7.5, p = 1, rbc = 0 |
|
Role functioning due to physical health |
85 (22.36) |
75 (25) |
t(4) = 0.784, p = 0.477, d = 0.351 |
W = 4.5, p = 0.586, rbc = 0.5 |
|
Bodily pain |
67.2 (21.41) |
74.4 (21.43) |
t(4) = -0.627, p = 0.565, d = -0.28 |
W = 6, p = 0.786, rbc = -0.2 |
|
General health |
71 (18.84) |
65 (15.41) |
t(4) = 1.395, p = 0.235, d = 0.624 |
W = 8.5, p = 0.269, rbc = 0.7 |
|
Physical health component |
50.106 (6.82) |
51.32 (6.46) |
t(4) = -0.287, p = 0.788, d = -0.128 |
W = 9, p = 0.813, rbc = 0.2 |
|
Mental health |
67.2 (18.42) |
68.8 (9.96) |
t(4) = -0.225, p = 0.833, d = -0.101 |
W = 6, p = 0.784, rbc = -0.2 |
|
Role functioning due to emotional state |
73.4 (43.45) |
86.8 (18.07) |
t(4) = -0.594, p = 0.585, d = -0.265 |
W = 2, p = 1, rbc = 0.333 |
|
Social functioning |
84.8 (10.40) |
97.4 (5.81) |
t(4) = -3.184, p = 0.033, d = -1.424 |
W = 0, p = 0.098, rbc = -1 |
|
Vitality |
66 (10.84) |
66 (14.75) |
t(4) = 0, p = 1, d = 0 |
W = 5, p = 1, rbc = 0 |
|
Mental health component |
51.489 (4.99) |
47.668 (3.91) |
t(4) = 3.318, p = 0.029, d = 1.484 |
W = 15, p = 0.063, rbc = 1 |
Note: integrated scales are shaded in grey; statistically significant differences (p < 0.05) are indicated in bold; marginally significant differences (p < 0.1) are indicated in italics.
As shown in Table 1, the overall ACE-III score increased following the intervention; however, the difference did not reach statistical significance. Nevertheless, the effect size was of a moderate magnitude (d = -0.671, rbc = -0.7). This suggests that, if the observed trend is not attributable to random variation, it may reach statistical significance in a larger sample. At the level of individual ACE-III subscales, a trend towards improvement was observed for Associative Processing Speed. The effect size was particularly large (rbc = -1): four of the five participants demonstrated an increase in their scores on this subscale, while no change was observed for the remaining participant. Conversely, a weaker but comparable effect in the opposite direction was observed for the Attention subscale (d = 0.539, rbc = 0.6), suggesting a potential decline in performance between the first and second assessment points. Thus, despite the overall tendency towards improvement in ACE-III scores, changes may have been heterogeneous across individual cognitive domains. A more detailed analysis of these patterns is an important direction for future research using a larger sample.
No significant differences were observed for the SF-36 physical health component scales. In contrast, scores on the Mental Health Component Summary increased, with a statistically significant difference detected using the t-test. At the level of individual scales, a significant improvement was observed for Social Functioning. The pattern was similar to that described above for Associative Processing Speed: four of the five participants demonstrated increased scores, while one participant showed no change. Notably, this participant had already achieved the maximum possible score at baseline.
Particular interest may lie in examining not only overall trends but also individual patterns of change in cognitive functioning among study participants. Figure 1 presents individual profiles for the overall ACE-III score, as well as for the Physical Health Component Summary and Mental Health Component Summary scales of the SF-36.
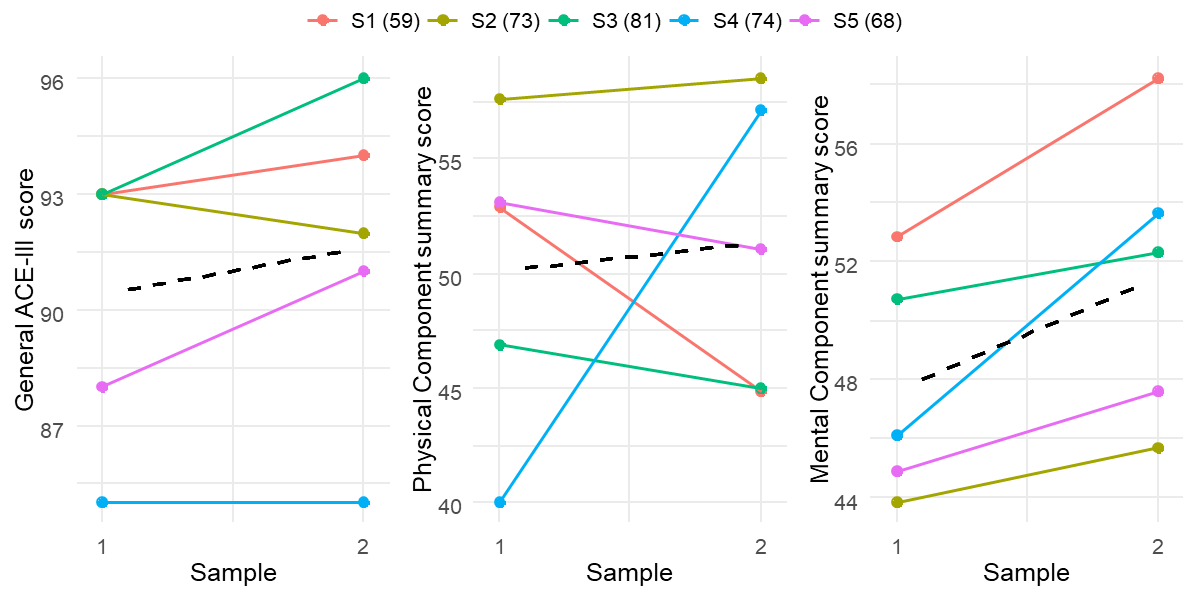
As shown in Figure 1, overall ACE-III scores increased in three of the five participants (although the increase for participant S1 was minimal), decreased in one participant (S2), and remained unchanged in another participant (S4). Notably, S4 was the only male participant in the sample and was older than the sample mean (74 years versus a mean age of 70.2 years). He also had the lowest ACE-III score in the group. Interestingly, participants S1, S2, and S3 had almost identical baseline ACE-III scores, yet demonstrated different trajectories of change. Participant S3 showed a substantial increase in score, S1 demonstrated a more modest improvement, whereas S2 exhibited a decline. Thus, these preliminary pilot data suggest that the effects of the programme on overall cognitive functioning may vary across subjects.
With regard to the Physical Health Component Summary, the greatest positive change was observed for participant S4, who had the lowest baseline score in the sample. Another participant (S2), who initially had the highest score on this measure, showed only a minimal increase. For the remaining participants, scores decreased between the first and second assessment points. Overall, the pattern is mixed. It may be hypothesised that improvements in the physical health component are more likely among subjects with lower baseline levels of physical health; however, this assumption requires further investigation in a larger sample.
Finally, a relatively consistent pattern was observed for the Mental Health Component Summary: this indicator increased, to varying degrees, in all study participants. The greatest improvements were observed for participant S4, who had a relatively low baseline score on this scale, and participant S1, who had the highest baseline score in the sample. This suggests that improvements associated with participation in the programme may occur among individuals with both relatively low and relatively high baseline levels of mental health.
Overall, the greatest heterogeneity in individual trajectories of change was observed for the Physical Health Component Summary (Figure 2). This may be attributable to differences in participants’ somatic health status. It should be noted that the programme was primarily designed to target cognitive and psychological aspects of health, which demonstrated a more consistent pattern of improvement between the first and second assessment points. Nevertheless, these findings highlight the importance of evaluating programme effectiveness in a larger and more representative sample.
To explore potential factors associated with participation in or withdrawal from the programme, baseline characteristics of participants who completed the programme and those who declined participation after the initial assessment were compared (n = 5 in each group). For the purposes of the analysis, these groups are referred to as the “participants” and the “non-participants”, respectively. Comparisons were conducted using three measures: the overall ACE-III score and the Physical and Mental Health Component Summary scores of the SF-36. The results are presented in Figure 2.
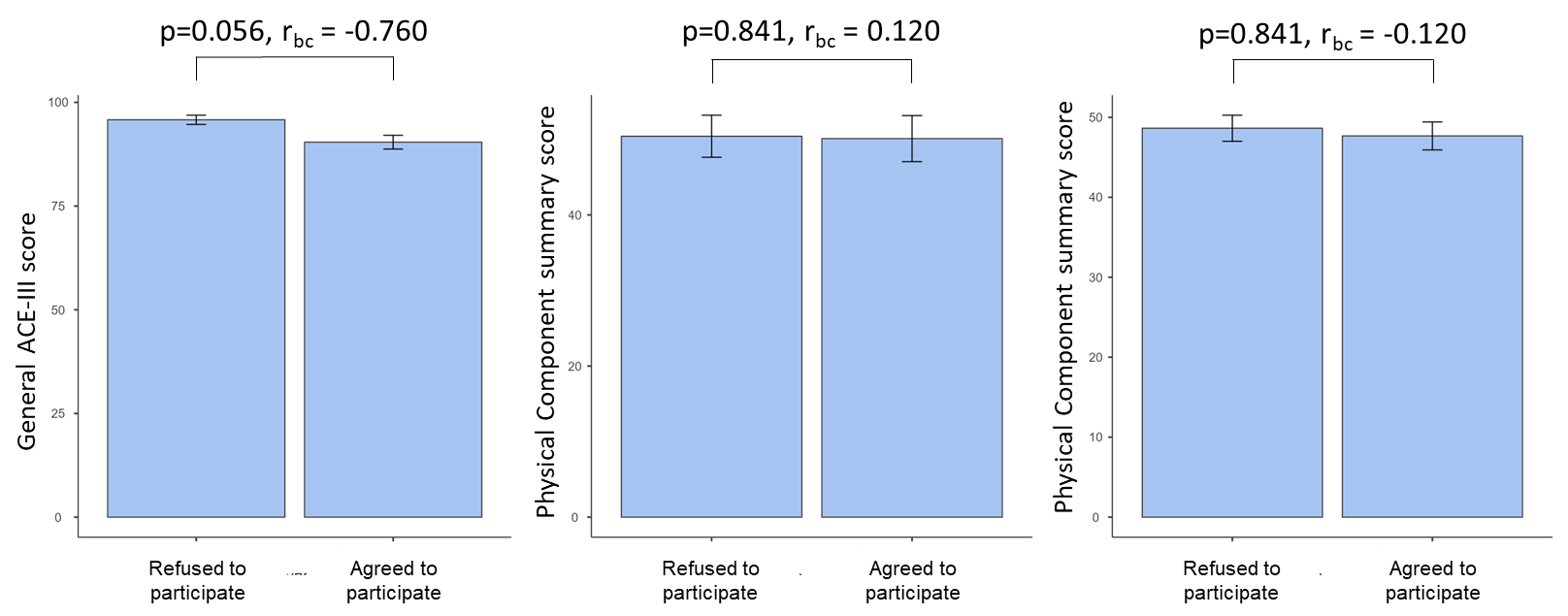
As shown in Figure 2, marginally significant differences were observed for the overall ACE-III score, with a higher mean score in the group of non-participants. These findings suggest that the overall level of cognitive functioning, as assessed by the ACE-III, may influence willingness to participate in the programme, with individuals demonstrating lower cognitive performance appearing more likely to enrol. No clear conclusions can be drawn regarding the SF-36 indicators. Differences between the groups were small and non-significant, and effect sizes were minimal. Moreover, the patterns observed for the Physical and Mental Health Component Summary scores were inconsistent, with effects occurring in opposite directions.
Thus, the overall level of cognitive functioning among study participants appears to have remained relatively stable. Nevertheless, individual cases demonstrated both improvements and declines in ACE-III scores and in the Physical Health Component Summary. It may be hypothesised that individuals with relatively lower baseline levels of these indicators, while still within the normative range, are more likely to demonstrate positive change following participation in the programme. However, this assumption requires further investigation in a larger sample. At the same time, despite the small sample size, a significant or near-significant improvement was observed for the Mental Health Component Summary of the SF-36. All programme participants demonstrated some degree of improvement on this measure. These findings suggest that the programme may positively influence participants’ overall psychological well-being, although confirmation of this effect will require replication in a larger sample.
With regard to the characteristics of participants who completed the programme and those who declined participation, the analysis indicated that programme participants tended to have relatively lower ACE-III scores, although still within the normative range. Given the small group sizes, however, this finding requires further verification and confirmation in future studies.
It would also be informative to compare changes between the first and second assessment points in the two groups — those who participated in the programme and those who declined participation. Such an analysis was not conducted in the present study because this design would typically require analysis of variance, which necessitates a substantially larger sample size. In the present study, follow-up data were available for only three subjects in the comparison group, further limiting its size. Analyses of this type should be considered when designing future studies.
Participant progress was monitored using four parameters: interest, communication, enjoyment, and mood. Interest was assessed based on the degree of participants’ cognitive engagement in individual activities and in the programme as a whole. Communication was evaluated with regard to the number of group members with whom the participant interacted during the session and the frequency of these interactions. Enjoyment was assessed based on participants’ responses to the session activities. Mood was evaluated as the participant’s overall emotional state throughout the session. Expert ratings were completed by the group facilitators after each session following a joint discussion of participants’ behaviour, general and communicative activity, emotional responses, and evaluative comments regarding both the current session and the programme as a whole. Ratings were made using a five-point scale ranging from 0 to 4, where 0 indicated the complete absence of the characteristic being assessed and 4 indicated its maximum expression (Roshchina et al., 2023).
Descriptive statistics for the four progress-monitoring parameters are presented in Table 2.
Table 2
Results of participant engagement monitoring in the Cognitive Stimulation Therapy (CST) programme
|
Engagement parameter |
Mean |
SD |
|
Interest |
3.95 |
0.07 |
|
Communication |
3.90 |
0.14 |
|
Enjoyment |
3.93 |
0.10 |
|
Mood |
3.95 |
0.07 |
As shown in Table 2, mean scores for all progress-monitoring parameters were close to the maximum possible values, indicating a high level of participant satisfaction and engagement with the programme. It is noteworthy that relatively low ratings (2–3 points) were recorded for two participants following the first session. Thereafter, participants consistently received near-maximum or maximum ratings across all monitored parameters after each session.
Analysis of the feedback questionnaires indicated a high level of acceptability of the CST programme among participants. Scores across all evaluated dimensions — including interest in the sessions, comfort of interaction, perceived benefit, and overall satisfaction — were close to the maximum possible values, reflecting a high level of engagement and a positive perception of the programme. For example, one participant commented: “I enjoyed it. Everyone was friendly towards one another”.
The high levels of engagement and retention were reflected not only in quantitative indicators (100% programme completion among enrolled participants), but also in participants’ subjective evaluations, which demonstrated sustained interest in the sessions and a positive attitude towards the programme format. Qualitative data further suggest that the social and communicative aspects of the intervention constitute an important component of its acceptability among older adults experiencing normative ageing. In particular, participants emphasised the value of group interaction and the positive emotional atmosphere of the sessions. This finding is consistent with the conceptualisation of CST as a multifaceted intervention that incorporates not only cognitive stimulation but also social stimulation. As one participant noted: “I liked everything. I enjoy being part of this group”.
At the initial stages of the programme, slightly lower ratings were observed in a small number of cases, which may reflect participants’ adaptation to the format of the sessions. For example, in response to the question “How much did you enjoy today’s session?”, participants commented: “I liked the session, but its purpose was not entirely clear to me. That is why I am giving it a 4” (the participant was referring to a five-point scale); “I am not yet sure how interesting it is. I am looking forward to the next sessions”. Subsequently, ratings stabilised at consistently high levels, suggesting that participants rapidly adapted to and accepted the programme format.
Qualitative analysis of participant comments suggests that the programme was generally perceived as intellectually stimulating, emotionally supportive, and socially meaningful. For example, one participant noted: “What I particularly enjoyed was communicating with the other participants — it felt like meeting with friends”. More broadly, activities characterised by a strong social, communicative, and emotional component appeared to elicit the greatest engagement. Similar comments were repeatedly expressed by different participants across multiple sessions: “The atmosphere is friendly. That is very pleasant”; “I enjoyed the communication”; “Talking with you is a real pleasure — you leave feeling energised”; “I enjoy communicating and experiencing positive emotions. Thank you”.
At the same time, participants demonstrated individual preferences regarding particular activities and differed in their perceptions of which sessions were more or less challenging and engaging. For example, following Session 5 (“Current Affairs”), one participant commented: “I would have liked the activities to be more intensive and challenging”. Notably, no similar critical comments were reported for any of the other sessions. Overall, participant feedback suggests that Session 5 elicited somewhat lower levels of interest compared to the other sessions.
Activities involving the retrieval of autobiographical memories, particularly those associated with distant life experiences and personally meaningful events, elicited the most positive responses from participants. Typical comments included: “Memories of childhood were my favourite part”; “Working with memories and revisiting childhood”; “Pleasant childhood memories”; and “Memories of old Moscow”. These findings suggest that engagement with autobiographical memory represents one of the key strengths contributing to the acceptability of CST in the context of normative ageing.
Another category of activities that generated considerable interest involved verbal associations and word-based games. Participants’ sustained engagement with these tasks was reflected both in their reactions during the sessions and in responses to the feedback questionnaires. In answer to the question “What did you like most?”, participants reported: “Chains of word associations”; “The word challenge”; “Coming up with words”; “Generating different associations”; and “Word games — they are exactly the kind of activity I enjoy”.
Competitive and game-based activities were among the most preferred formats. As reflected in the feedback questionnaires, participants commented: “I enjoy all kinds of competitions and quizzes”. Creative activities were also consistently identified as particularly enjoyable: “Creativity is wonderful!”; “Working with natural materials was delightful”; and “Creative activities”.
Topics that carried personal relevance, involved discussion of real-life experiences, or incorporated visual and sensory elements tended to be received most positively. Several themes appeared to generate particularly high levels of interest among participants:
- Moscow (history, photographs, and orientation tasks): “The old photographs of Moscow were particularly interesting”; “The orientation activities related to Moscow were my favourite”.
- practical topics: “Money and how to use it is highly relevant”; “Comparing prices of different items”;
- sensory and guessing activities: “Guessing objects placed on the table while blindfolded”.
According to participants’ feedback, the core elements contributing to the programme’s appeal were sessions involving autobiographical reminiscence, word-based games, orientation activities, and creative tasks.
At the same time, several areas for further programme development can be identified. These include the need to provide a higher level of cognitive challenge for some participants and to more clearly explain the underlying principles of the intervention, particularly the distinction between cognitive stimulation and cognitive training. Thus, the acceptability of CST among cognitively healthy older adults appears to be determined not so much by its training component as by the broader social experience it provides to participants.
Description of the Intervention Implementation
In the present study, the CST programme was implemented in accordance with the core methodological recommendations (Roshchina et al., 2023), while incorporating modifications to the activities and stimulus materials. These adaptations were intended to increase the cognitive demands, variety, and complexity of the exercises, as well as to enhance their personal relevance and meaningfulness for older adults experiencing normative ageing.
The need for such modifications is supported by several considerations. Research has shown that, in populations experiencing normative ageing, a key determinant of engagement with and acceptance of an intervention is the perceived relevance of its content and its connection to participants’ personal experiences. Programmes incorporating autobiographical, socially meaningful, and emotionally engaging elements are perceived as more relevant and are more likely to sustain long-term engagement (Velloso et al., 2025). In addition, studies of cognitive interventions indicate that the greatest benefits are associated with activities requiring the active use of flexible and multidimensional problem-solving strategies, rather than the simple repetition or training of isolated skills (Lampit, Hallock, Valenzuela, 2014; Mowszowski et al., 2016). Accordingly, there is a need to increase both the variety and complexity of activities when adapting such programmes for older adults experiencing normative ageing.
The modifications introduced in the present study affected all standard components of the CST sessions, including the introductory, main, and closing sections.
During the introductory phase, participants were asked, as part of the time orientation activity, to generate symbolic and associative representations of the current date. During the ball game activity, participants completed tasks semantically related to the theme of the session, with three to four tasks presented in order of increasing difficulty. With regard to the discussion of current events, it was decided to move away from contemporary news coverage and instead focus on topics related to art, science, technology, urban development, and examples of unusual or noteworthy human achievements. Discussions of news items were accompanied by an evaluation of source credibility and consideration of indicators of information reliability.
The complexity of activities in the main part of each session was increased by reducing stimulus presentation time, increasing the pace of task performance, and introducing additional instructions in the form of competing tasks. The stimulus materials used in the main activities were also modified by incorporating less frequent and more complex stimuli, as well as by increasing the number and diversity of associative links. These links were expanded both within a single semantic field and through the integration of stimuli across multiple semantic domains.
At the participants’ request, the singing activity traditionally included in the closing section of the session was omitted. At the same time, the feedback component was expanded to include discussion of the factors that contributed to difficulties encountered during task performance and the effectiveness of strategies used to overcome them.
Specific modifications to the activities and techniques employed in the programme are presented in the Appendix table.
Discussion
The findings of the present pilot study suggest that the feasibility of Cognitive Stimulation Therapy (CST) in the context of normative ageing should be considered a multidimensional construct encompassing not only implementation-related indicators (recruitment, retention, and attendance), but also participants’ subjective perceptions of the programme and its potential cognitive and psychosocial effects.
Acceptability and Subjective Evaluation of the Programme (RQ1)
The present pilot study was designed to evaluate the feasibility of Cognitive Stimulation Therapy (CST) in a sample of older adults experiencing normative ageing and to obtain preliminary data regarding its potential effects. The findings can be discussed with reference to three key aspects: participants’ subjective evaluation of the programme, its potential cognitive and psychosocial effects, and possible directions for intervention optimisation.
The results indicate a high level of acceptability of CST among older adults experiencing normative ageing. Participants reported high levels of satisfaction with the programme (mean score = 3.93 out of 4), and participant retention reached 100%, indicating a high degree of engagement. These findings are consistent with studies of CST conducted in clinical populations, where the programme has likewise demonstrated high acceptability and retention rates (Aguirre et al., 2013; Orrell et al., 2017).
At the same time, it is important to note that the nature of programme acceptability in a normative ageing population appears to differ from that observed in clinical samples. Whereas cognitive benefits are often considered the primary outcome in clinical populations, the social and communicative component emerged as particularly salient in the present study. Participants consistently emphasised the importance of the group atmosphere and interpersonal interaction. We attribute this finding, at least in part, to the core principles of CST, according to which facilitators are encouraged to avoid a directive interaction style, and sessions are intended to take place in a positive, supportive, and accepting environment (Roshchina et al., 2023). Positive social support has been identified as a protective factor against cognitive decline in later life (Khondoker et al., 2017).
Thus, in the context of normative ageing, CST appears to function not only as a cognitive intervention but also as a setting that promotes emotional engagement and supports social participation. This interpretation is consistent with contemporary views on the role of social inclusion as a contributor to cognitive reserve and a protective factor against cognitive decline (Velloso et al., 2025).
Preliminary Effects on Cognitive Functioning and Quality of Life (RQ2)
The findings suggest limited but directionally consistent effects of the programme. These results may be interpreted in light of contemporary perspectives on the heterogeneity of cognitive ageing and individual differences in compensatory strategies, according to which intervention-related changes may emerge primarily at the level of specific cognitive processes rather than global cognitive status (Prince et al., 2024).
No statistically significant changes were observed in overall ACE-III scores. This finding is not unexpected given the normative level of cognitive functioning and the high baseline performance observed in the sample, which may have resulted in a ceiling effect. Similar limitations have been reported in studies of cognitive interventions involving cognitively healthy older adults (Velloso et al., 2025b).
Nevertheless, a trend-level increase in associative processing speed and moderate-to-large effect sizes (with rbc values reaching -1) warrant particular attention. These findings suggest that CST may primarily influence dynamic aspects of cognitive functioning, such as verbal fluency and associative processing, rather than global cognitive status. Improved processing speed has been identified as a protective factor against age-related cognitive decline (Coe et al., 2026). At the same time, dynamic characteristics of cognitive performance are closely linked to metacognitive processes (Hulbig, 2026).
The most consistent effects were observed in the domain of psychosocial functioning, including a significant improvement in social functioning and a significant improvement in the mental health component of quality of life. In contrast, no changes were observed in the physical health component, which is consistent with theoretical expectations, as CST is not designed to target physical or somatic functioning.
Importantly, improvements in mental health indicators were observed in all participants, regardless of their baseline levels. This finding suggests that CST may exert its primary effects on subjective well-being, emotional functioning, and social inclusion.
These results are consistent with evidence from meta-analyses indicating that, in non-clinical populations, cognitive stimulation interventions tend to produce more pronounced effects on psychosocial outcomes than on cognitive measures (Gómez-Soria et al., 2023; Velloso et al., 2025b).
Directions for Programme Optimisation (RQ3)
Analysis of participant feedback allows several key directions for adapting CST to cognitively healthy older adults to be identified:
- varying task difficulty through the introduction of additional cognitively demanding activities (“challenge” tasks);
- repositioning the programme from a therapeutic intervention towards a framework of active and healthy ageing, with an emphasis on development and maintenance rather than remediation;
- preserving and further strengthening the core components that constitute the programme’s stable “active ingredients”: autobiographical memory activities, verbal and associative tasks, game-based and competitive formats, and opportunities for social interaction.
Thus, the effectiveness of the programme appears to be associated not with any single activity, but rather with the combination of sensory, cognitive, social, and emotional stimulation it provides. This interpretation is fully consistent with the core principles underlying Cognitive Stimulation Therapy (Roshchina et al., 2023).
An important finding of the present study is the discrepancy between the high levels of acceptability and engagement observed among enrolled participants and the selective feasibility of recruitment, reflected in the relatively high refusal rate (50%). Reasons for declining participation — including unmet expectations, lack of perceived need, and logistical barriers — suggest that the feasibility of CST depends not only on the characteristics of the programme itself, but also on how it is presented, the extent to which it aligns with participants’ expectations and perceived needs, and the organisational conditions under which it is delivered. This finding broadens the understanding of feasibility and is consistent with contemporary implementation frameworks, particularly the Consolidated Framework for Implementation Research (CFIR), which conceptualises implementation success as the result of interactions among intervention characteristics, participant characteristics, implementation context, and organisational factors. Within the CFIR framework, the present findings may be interpreted as reflecting the influence of several domains simultaneously: intervention characteristics (e.g., perceived complexity and alignment with expectations), participant characteristics (e.g., motivation and perceived need), and organisational context (e.g., accessibility and logistical considerations). Accordingly, the observed selectivity in participant recruitment highlights the importance of considering implementation-related factors already at the stage of adapting CST for populations experiencing normative ageing (Damschroder et al., 2009).
Similarly, within the logic of the RE-AIM framework, both reach and implementation feasibility are understood to depend substantially on the accessibility of an intervention and its perceived relevance to the target population (Glasgow, Vogt, Boles, 1999). From this perspective, the observed selectivity in recruitment may be interpreted as an indicator of a limited alignment between programme characteristics and the expectations of some potential participants.
The present findings are also consistent with the concept of the acceptability of healthcare interventions and the Theoretical Framework of Acceptability (TFA), which emphasise that the perceived acceptability of an intervention is determined not only by its content but also by the extent to which it is viewed as appropriate, aligned with participants’ expectations, and personally meaningful (Sekhon, Cartwright, Francis, 2017).
Thus, the feasibility of CST in the context of normative ageing may be conceptualised as the outcome of alignment across three levels: the characteristics of the intervention itself, the characteristics of the target population, and the implementation context. This highlights the importance of considering implementation-related factors already at the stage of programme adaptation and positioning.
Power Analysis
To inform future research based on the preliminary findings of the present study, a power analysis was conducted to estimate the minimum required sample size. The observed effect sizes may be considered moderate to large; however, a conservative effect size estimate (specifically, d = 0.5) was adopted for planning purposes. Assuming a statistical power of 0.8 and a significance level of α = 0.5, the minimum sample size required to obtain reliable results using a paired-samples t-test (i.e., comparing two assessment points) was estimated at 35 participants. To achieve a power level of 0.95, a sample of 57 participants would be required.
A sample size calculation was also performed for the full study design, including experimental and control groups assessed at two time points (pre- and post-intervention), using a mixed-design analysis of variance. Assuming a small expected effect size (f = 0.25), a moderate correlation between assessment points (r = 0.30), a significance level of α = 0.5, and statistical power of 0.8, the recommended minimum sample size was 46 participants (23 participants in each group). Increasing the target power to 0.95 yielded a recommended sample size of 76 participants (38 participants per group).
Conclusion
In summary, the CST programme demonstrated high feasibility in a sample of older adults experiencing normative ageing. Retention (100%), attendance (Me = 11 of 14 sessions), and satisfaction ratings (approximately 3.9–4.0 out of 4) indicate a high level of programme acceptability in this population. This finding is particularly important given that participants did not present with clinical impairments and were able to maintain their usual lifestyles throughout the intervention.
In the context of normative ageing, substantial improvements in ACE-III scores are difficult to expect because of ceiling effects associated with high baseline performance (85–93 out of 100). Nevertheless, improvements in overall scores were observed in three of the five participants, while four of the five participants demonstrated stable or improved performance across attention and memory domains. The effect sizes estimated using rank-biserial correlation suggest the potential presence of moderate-to-large effects.
Individual trajectories indicate overall stability of cognitive functioning in normative ageing, accompanied by moderate improvements in some participants and the most consistent positive changes in the mental health component of quality of life.
These findings suggest that CST may serve as a supportive cognitive intervention in the context of normative ageing. However, confirmation of its effectiveness will require a randomised controlled trial.
Overall, the results indicate that CST is both a feasible and acceptable intervention for cognitively healthy older adults.
The findings further support the view that CST may be considered not only as a therapeutic approach for cognitive impairment, but also as a model of structured cognitive and social activity within the framework of active ageing.
Limitations. Despite the significance of the findings, several key limitations should be considered when interpreting the results and applying them to broader contexts.
Non-randomised design. The CST programme was implemented within a pilot study framework, which limits the ability to control for potential biases arising from selective recruitment. The groups were formed naturally, and participants self-selected into participation, which may have introduced selection effects.
Small sample size. The sample size (N = 10) substantially limits the generalisability of the findings to broader populations of older adults with normative ageing. With such a sample size, the statistical power of the study is limited, constraining the reliability of the observed effects and rendering conclusions preliminary. A small sample also reduces the sensitivity of the study to detect more subtle differences in cognitive and psychosocial outcomes, particularly in the presence of ceiling effects on cognitive measures (Velloso et al., 2025b). Furthermore, the limited sample size precluded the use of more advanced statistical approaches, such as multivariate analyses or subgroup comparisons.
Lack of longitudinal follow-up. The study included only a single intervention cycle, which restricts the ability to assess the durability of the observed effects. Short-term improvements, such as enhancements in psychological well-being and social aspects of quality of life, do not necessarily indicate sustained effects over time. This highlights the need for studies incorporating longer follow-up periods.
Limited implementation context. All sessions were conducted within a single institutional setting under fixed organisational conditions, which limits the generalisability of the findings to other settings and contexts. This underscores the importance of implementation research, including the application of frameworks such as the Consolidated Framework for Implementation Research (CFIR), to examine organisational, cultural, and contextual factors influencing the successful implementation of CST across different settings and populations.
1 World Health Organization. (2022). Ageing and health. URL: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (viewed: 22.03.2025).
2 Alzheimer’s Disease International. (2023). World Alzheimer Report 2023. URL: https://www.alzint.org/resource/world-alzheimer-report-2023/ (viewed: 22.03.2026).
3 World Health Organization. (2015). World report on ageing and health. URL: https://iris.who.int/server/api/core/bitstreams/5174879e-b0dc-43fc-b3a8-b1db31c51d4c/content (viewed: 22.03.2026).
4 World Health Organization. (2019). Risk reduction of cognitive decline and dementia: WHO guidelines. URL: https://www.ncbi.nlm.nih.gov/books/NBK542796/ (viewed: 21.02.2026).
5 Russian Association of Gerontologists and Geriatricians, Russian Society of Psychiatrists. (2020). Cognitive disorders in elderly and senile persons: clinical guidelines. URL: https://psyrus.ru/med_psy/klinicheskie-rekomendatsii/kognitivnie_rasstroistva_pogilie_1204202.pdf (viewed: 21.03.2026).